Downloaded 218 times


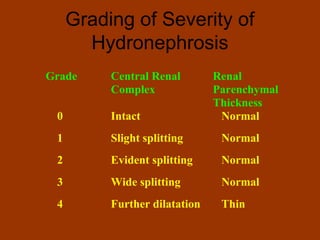

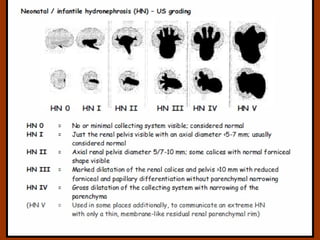
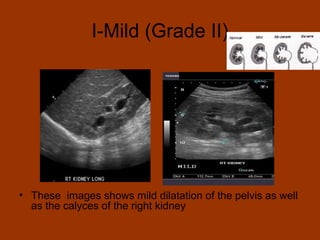
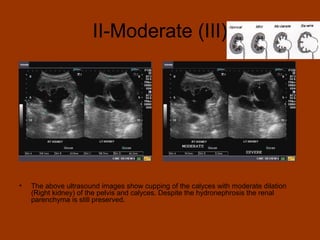
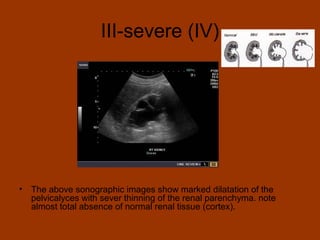
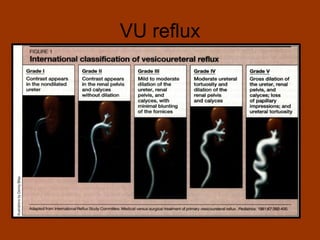
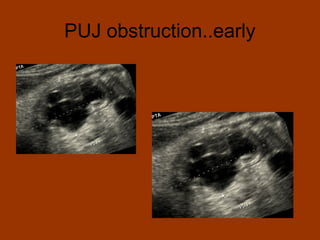
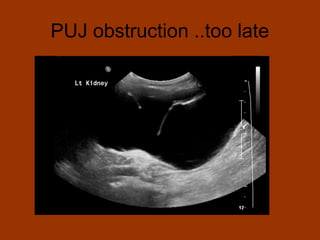

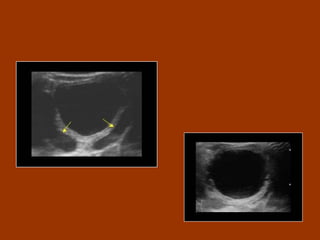
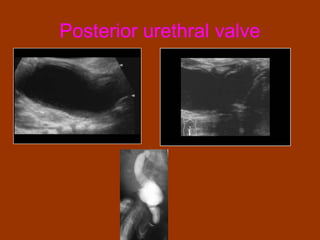

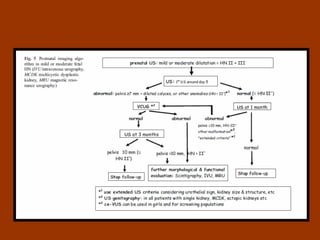


The document discusses the significance of fetal hydronephrosis, a common congenital condition identified via antenatal ultrasonography, which can indicate conditions such as ureteropelvic junction obstruction that may require surgical intervention. A grading system for hydronephrosis in fetuses is established, highlighting that grades I and II may be benign, while grades IV and V generally necessitate surgery. It emphasizes the need for careful evaluation and monitoring of significant dilatations to prevent permanent kidney loss.
























![Paediatric Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/paeduroedmond-140716213023-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
