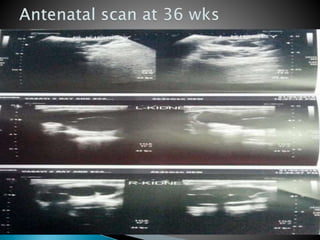
This document describes the case of a 4-day old male neonate admitted to the hospital for evaluation of antenatally detected bilateral hydronephrosis. The baby was delivered full-term via normal vaginal delivery and initial examinations were normal. Antenatal ultrasounds showed progressively worsening bilateral hydronephrosis. Postnatal ultrasound confirmed bilateral hydronephrosis more severe on the left side. Laboratory tests and renal function were normal. A micturating cystourethrogram detected bilateral vesicoureteral reflux grade 3 on the right and grade 2 on the left. The baby received antibiotics and was discharged with instructions to follow-up in one month and continue prophylactic medications.





![ Behrman, R.E., Kliegman, R.M., & Jenson, H.B. (2000).
Nelson Textbook of Pediatrics (16th ed.). Page1445-1454.
Indian Pediatrics 2001; 38: 1244-1251
Consensus Statement on Management of Antenatally Detected
Hydronephrosis.
Indian J Nephrol. 2013 Mar-Apr; 23(2): 83–97.
. Mallik M, Watson AR. Antenatally detected urinary tract
abnormalities: More detection but less action.Pediatr
Nephrol. 2008;23:897–904. [PubMed]
2. Dudley JA, Haworth JM, McGraw ME, Frank JD, Tizard EJ.
Clinical relevance and implications of antenatal
hydronephrosis. Arch Dis Child Fetal Neonatal
Ed. 1997;76:F31–4. [PMC free article] [PubMed]
Goole images](https://image.slidesharecdn.com/vurreflex-150622021833-lva1-app6891/85/Vur-reflex-35-320.jpg)










































































