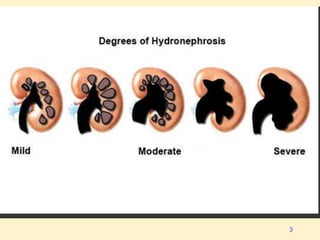
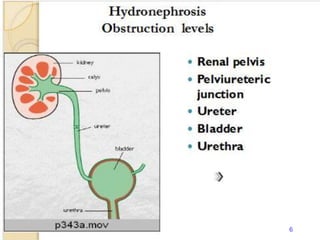
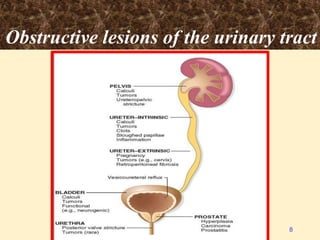
Hydronephrosis is the dilation of the renal pelvis and calyces due to urine obstruction, leading to kidney damage. It can occur from various causes, including congenital anomalies, urinary calculi, and tumors, with the effects varying from acute to chronic conditions. Diagnosis involves imaging studies, and treatment may be non-operative or require surgical intervention depending on the severity and symptoms.