Downloaded 54 times
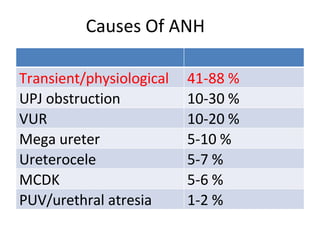
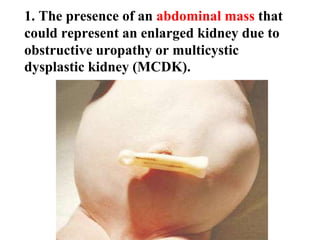

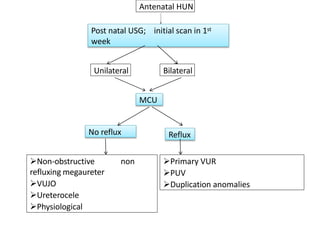

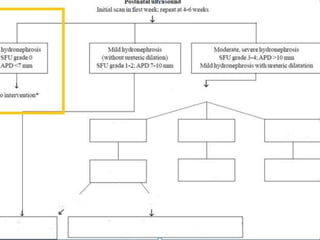
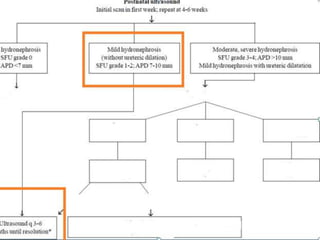
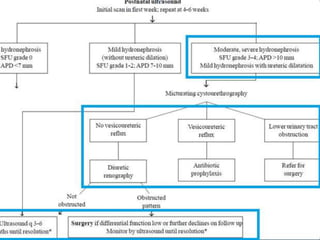


The document discusses the management of neonatal hydronephrosis, detailing causes, diagnostic evaluation, and treatment options. It highlights the importance of antenatal and postnatal ultrasound for assessing urinary tract anomalies and outlines guidelines for follow-up investigations such as voiding cystourethrography and renal scans. Management strategies, including indications for surgery and the use of prophylactic antibiotics, are also covered, emphasizing the need for careful evaluation of hydronephrosis severity and associated risks.


























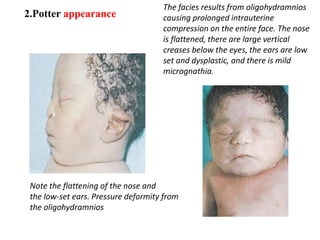
![Paediatric Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/paeduroedmond-140716213023-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)








































