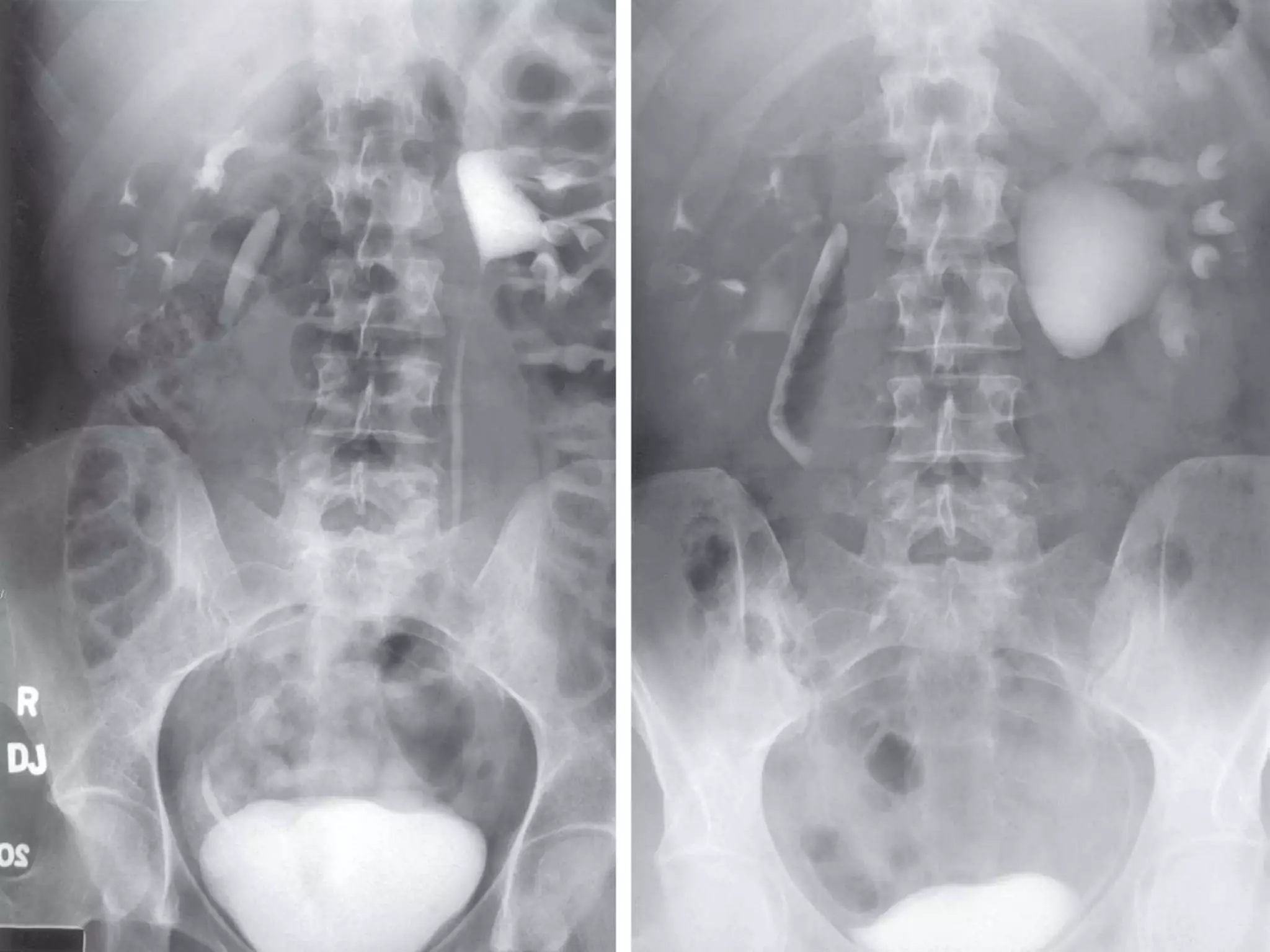
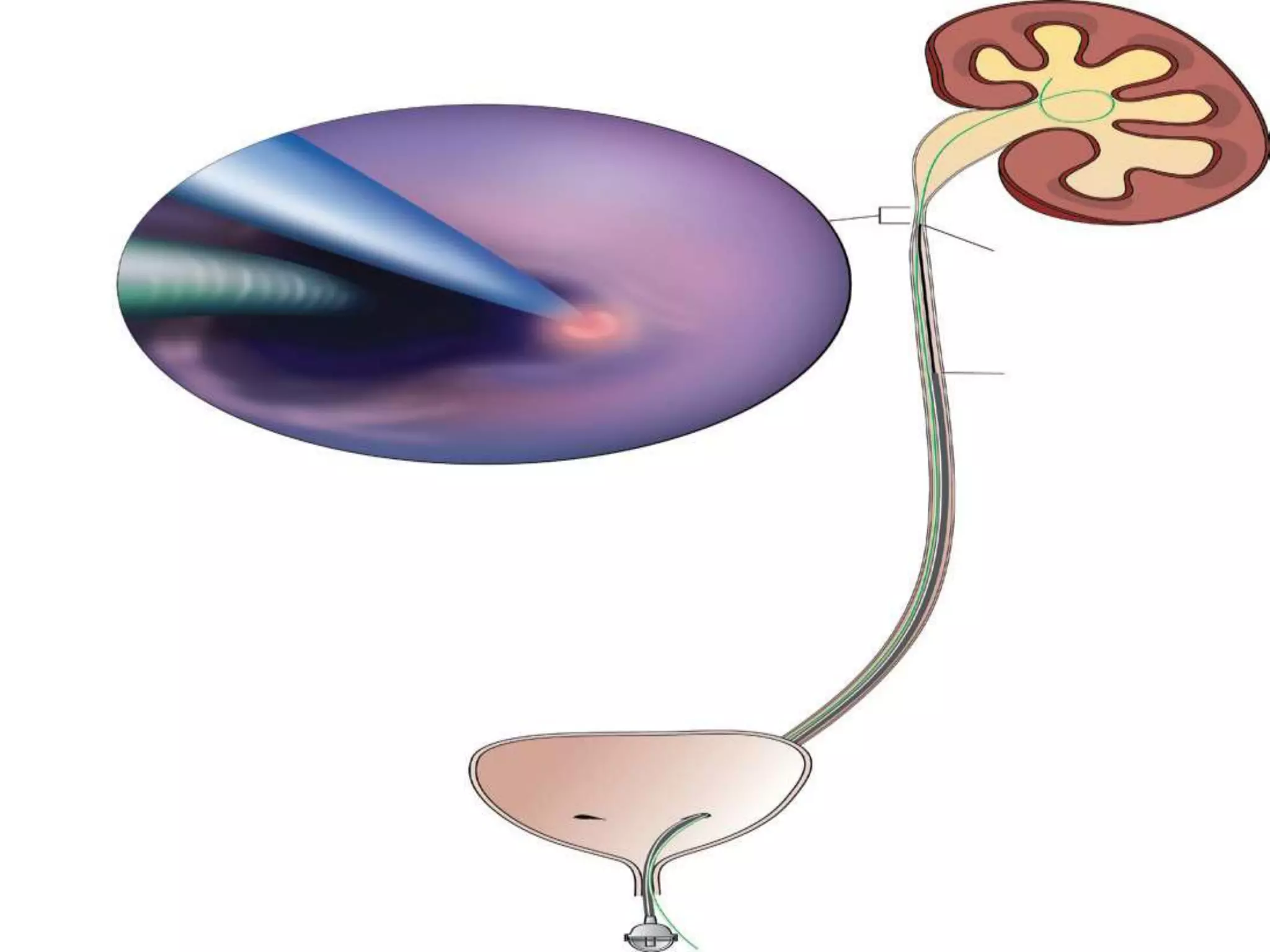
The ureters are tubular structures that transport urine from the kidneys to the bladder. They have multiple layers including epithelium, smooth muscle, and adventitia. Sites of natural narrowing include the ureteropelvic junction (UPJ) and ureterovesical junction. UPJ obstruction is most common in boys and on the left side. It can be caused by intrinsic narrowing at the UPJ or extrinsic compression. Surgical intervention is considered if renal function declines or symptoms develop. Treatment options include open or laparoscopic pyeloplasty, endopyelotomy, or ureterocalycostomy depending on the specifics of each case.