Downloaded 29 times

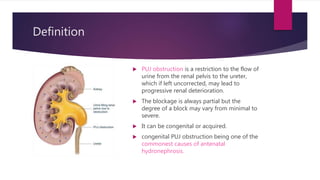


PUJ obstruction is a restriction of urine flow from the renal pelvis to the ureter. It can be congenital or acquired, with congenital being one of the most common causes of antenatal hydronephrosis. Diagnosis involves ultrasonography, VCUG, diuretic renography and other imaging modalities to determine severity and presence of associated issues. Treatment depends on severity but typically involves surgical intervention like open or laparoscopic pyeloplasty to resect and reanastomose the obstructed segment if drainage is significantly impaired or renal growth is poor. Postoperative follow up with imaging is important to monitor repair.



































































