This document discusses ectopic ureters and ureteroceles. Some key points:
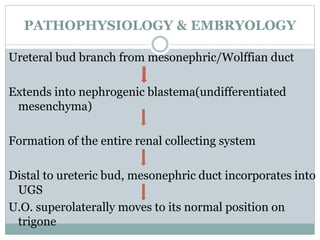
1. Ectopic ureters and ureteroceles are congenital abnormalities that occur due to abnormal development of the ureter and urinary tract.
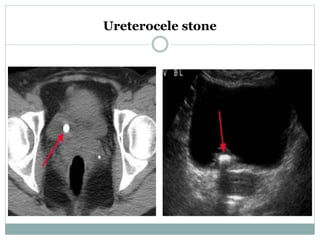
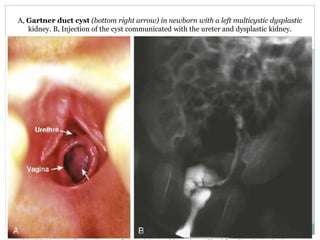
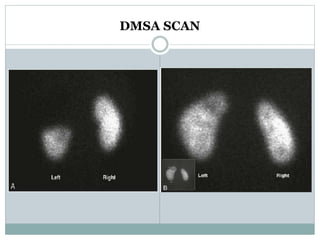
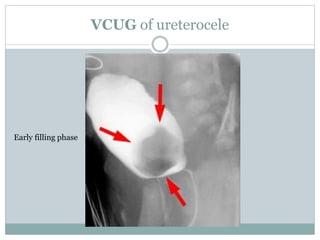
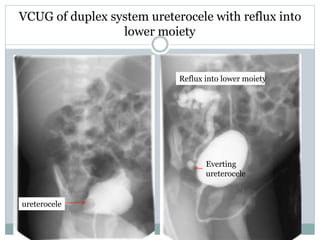
2. Clinical presentations can include urinary tract infections, incontinence, pain, and obstruction. Evaluation involves ultrasound, voiding cystourethrogram, nuclear scans, and possibly MRI.
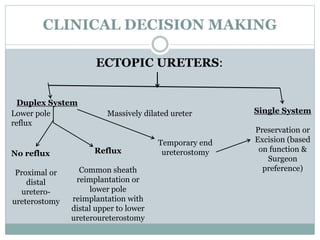
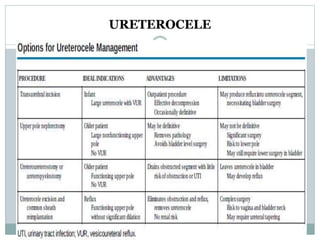
3. Management depends on factors like obstruction, reflux, and renal function. Options include observation, acute decompression, definitive surgery like reimplantation, and in some cases total reconstruction or upper pole nephrectomy. Complications