Downloaded 11 times


![The pathology underlying atypical flutter is highly variable, and
these circuits may occur in the context of
(1) Prior corrective atrial surgery (congenital heart disease [CHD],
valvular heart disease, after a Maze procedure or cardiac
transplantation),
(2) Previous AF ablation,
(3) Advanced atrial disease associated with atrial enlargement
(these patients frequently have underlying pathologies such as
heart failure [systolic or diastolic] or unoperated valvular heart
disease such as severe mitral regurgitation),
(4) In patients with normal atrial size and without an obvious
underlying pathologic condition. In these patients, spontaneous
scarring of unknown cause may be found at the time of atrial
mapping. These circuits have particularly been described in the RA
free wall.](https://image.slidesharecdn.com/narrowcomplextachycardia-220821072544-122aba3a/85/NARROW-COMPLEX-TACHYCARDIA-pptx-88-320.jpg)

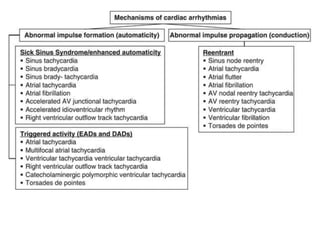
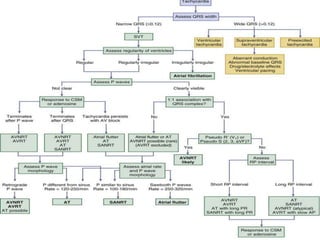
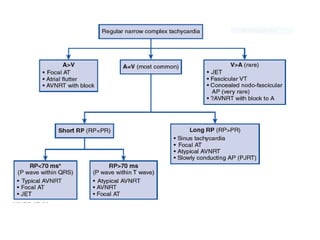
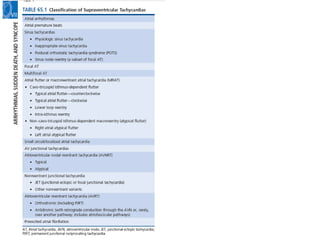
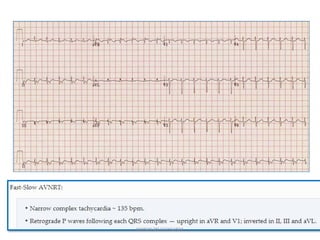
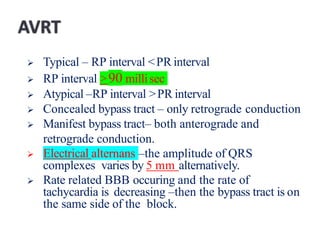
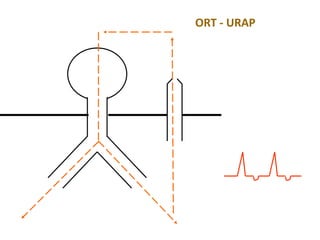
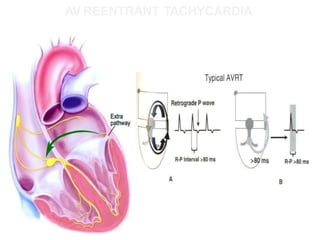
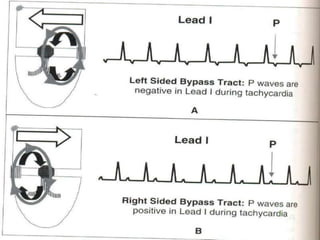
1. This document discusses the approach to evaluating and diagnosing narrow complex tachycardias. It describes the main mechanisms that can cause tachycardias including enhanced automaticity, triggered activity, and reentry. 2. Specific tachycardia types are then discussed in detail including AV nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT), atrial tachycardia (AT), junctional ectopic tachycardia (JET), and inappropriate sinus tachycardia. The diagnostic criteria and distinguishing characteristics of each are provided. 3. A number of other arrhythmias are also briefly covered such























































































