![Presented by:
Trilochan pandey, Romit Subba, Harif Ghimire, Mamata Panthi,
Arunima Shrestha [B.Pharmacy II year]](https://image.slidesharecdn.com/acasestudyonarrythmia-160910134922/85/case-study-on-arrythmia-1-320.jpg)



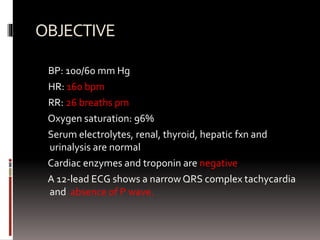
![ASSESMENT
ECG characteristics like absence of P waves and irregular
R-R intervals due to irregular conduction of impulses to
ventricles diagnosed atrial fibrillation(A-Fib)
Initial goal of treatment is to slow his HR. A CCB is drug
of choice,slows conduction and increases refractoriness
To prevent thromboembolic events such as CVA, Heparin
and warfarin should be given. IV heparin drip should be
given until warfarin reaches a therapeutic serum
level[PT/INR and PTT monitoring must be set up]](https://image.slidesharecdn.com/acasestudyonarrythmia-160910134922/85/case-study-on-arrythmia-7-320.jpg)
![PLAN
INPATIENT
o 20mg Diltiazem is given by IV push
[In response, pt. HR slowed to 120bpm bt rapidly returned
to high rate]
o After 15 mins, another bolus was ordered, followed by
continuous IV infusion of diltiazem at 5mg/hr[can be
titrated upto 15mg/hr to achieve desired rate]
After 1-2 hrs on diltiazem drip, pt. HR drops to 80-90bpm
o A Heparin drip is started along with oral warfarin 2mg
[PT/INR and PTT is ordered]](https://image.slidesharecdn.com/acasestudyonarrythmia-160910134922/85/case-study-on-arrythmia-8-320.jpg)




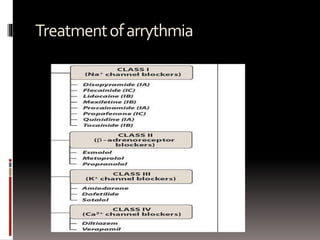
The document discusses arrhythmias, characterized by irregular heartbeat and caused by abnormalities in cardiac activation. It covers various types including atrial fibrillation, atrial flutter, and sinus arrhythmia, among others, and outlines a clinical case involving a patient with atrial fibrillation treatment using diltiazem and anticoagulants. Treatment goals focus on heart rate control and prevention of thromboembolic events, alongside patient education regarding lifestyle modifications.























































































