Downloaded 16 times







![[Micro] syphilis](https://image.slidesharecdn.com/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892/85/Micro-syphilis-54-320.jpg)
![[Micro] syphilis](https://image.slidesharecdn.com/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892/85/Micro-syphilis-55-320.jpg)
![[Micro] syphilis](https://image.slidesharecdn.com/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892/85/Micro-syphilis-56-320.jpg)

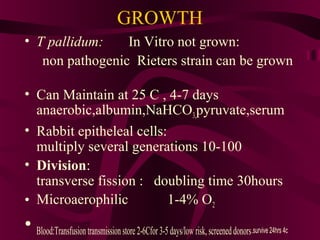
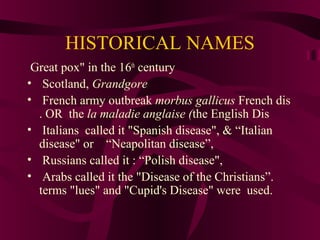
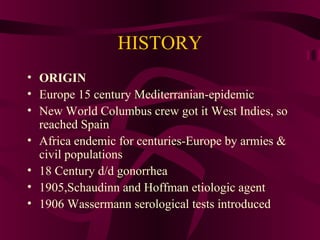
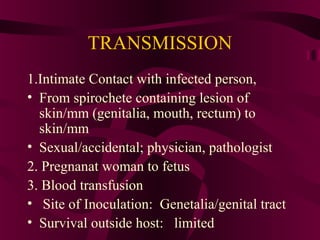
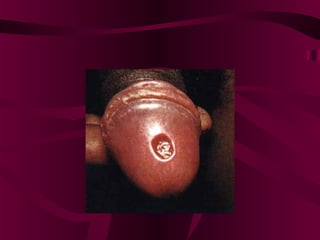
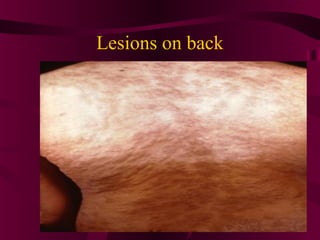
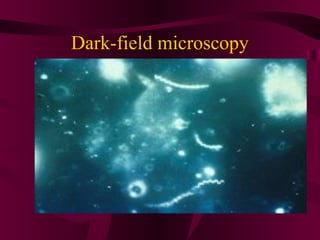
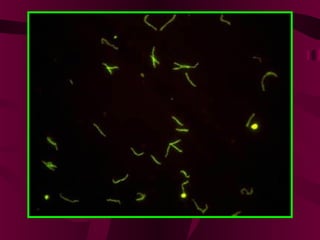
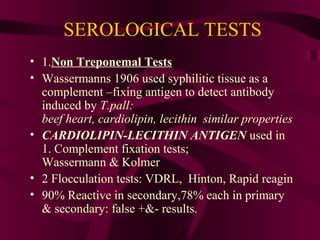
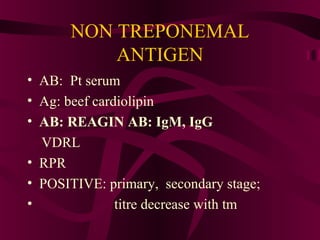
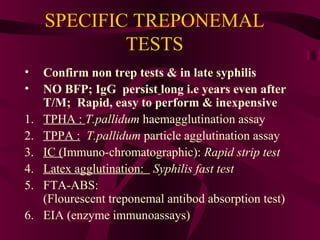
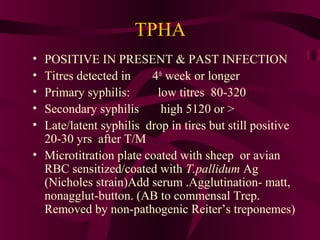
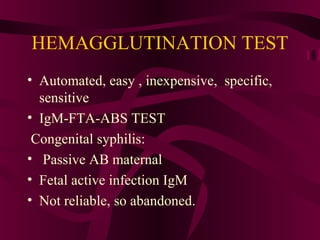
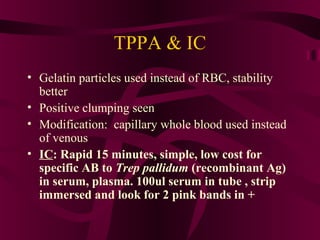
This document provides information on the bacteria Treponema pallidum, which causes syphilis. It discusses the morphology, structure, growth, transmission and pathogenesis of T. pallidum. It also summarizes the clinical manifestations and stages of syphilis, including primary, secondary, latent and tertiary syphilis. Laboratory methods for diagnosis are outlined, including darkfield microscopy, serological tests such as the non-treponemal tests (VDRL, RPR) and treponemal tests (TPHA, FTA-ABS).




























![[Int. med] jugular venous pressure from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/ttnn2w5hsv594ygpbtvp-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171701-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)

![[Micro] pathogenesis](https://cdn.slidesharecdn.com/ss_thumbnails/micropathogenesis-150502144426-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)









![[Pharma] 1.sources of drug & active principles](https://cdn.slidesharecdn.com/ss_thumbnails/pharma1-150502144439-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




![[Micro] chemical sterilizaton](https://cdn.slidesharecdn.com/ss_thumbnails/xwi6imyrrchg97geohxj-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

![[Behv. sci] stress management by SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/cltz4ljwt3knztztzeem-signature-413e8c33574c21294a6dc95e37151f54f981375d6b0f4695b85074f597ea60c2-poli-150813085608-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![Syphilis new.pptx [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/syphilisnew-190407075658-thumbnail.jpg?width=640&height=640&fit=bounds)



















![[Micro] sterilization](https://cdn.slidesharecdn.com/ss_thumbnails/jtli2uutrkcchg3xbjaw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] mycobacterium tuberculosis](https://cdn.slidesharecdn.com/ss_thumbnails/knwspassdmixhofx5ycy-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] pathogenesis](https://cdn.slidesharecdn.com/ss_thumbnails/reicxvotaytkxx8xnaam-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] parvovirus](https://cdn.slidesharecdn.com/ss_thumbnails/9efvufm6tsedx9o58t7q-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] hymenolepis nana](https://cdn.slidesharecdn.com/ss_thumbnails/3rxjz7ekrwinb1sq3uxs-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] gram positive spore bearing rods](https://cdn.slidesharecdn.com/ss_thumbnails/xi8ojr00samkfuo2qtsz-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] opportunistic mycosis](https://cdn.slidesharecdn.com/ss_thumbnails/r9htdghqrikznf5hrtly-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] mycobacterium leprae](https://cdn.slidesharecdn.com/ss_thumbnails/i6vamgi4rq2srkk4yof7-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] aspergillus](https://cdn.slidesharecdn.com/ss_thumbnails/f74upwejq4u9rqvunxal-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] growth and culturing of bacteria](https://cdn.slidesharecdn.com/ss_thumbnails/xfkdsyhfs92guomky6hu-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] classification of prokaryotes](https://cdn.slidesharecdn.com/ss_thumbnails/6kp4xq4eqt6dbdni5yhj-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] clostridia](https://cdn.slidesharecdn.com/ss_thumbnails/rosblh0htbiwcq9fv3y4-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial genetics (6 jan)](https://cdn.slidesharecdn.com/ss_thumbnails/capdzkrqktd9kgwl1skw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial selective & differential media](https://cdn.slidesharecdn.com/ss_thumbnails/inykegaks3iuut4oc1pw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] cestodes](https://cdn.slidesharecdn.com/ss_thumbnails/nvpl1fbyq2ofjfsbmped-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] atypical mycobacterium](https://cdn.slidesharecdn.com/ss_thumbnails/7d5djanirg26boloifek-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial genetics (12 jan)](https://cdn.slidesharecdn.com/ss_thumbnails/ybiw66hrget4bdnxz447-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] adenoviruses](https://cdn.slidesharecdn.com/ss_thumbnails/rqzzph7ktam2nsjysnxg-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] actinomyces](https://cdn.slidesharecdn.com/ss_thumbnails/9ecmrhoqrkocvbxkfudx-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
