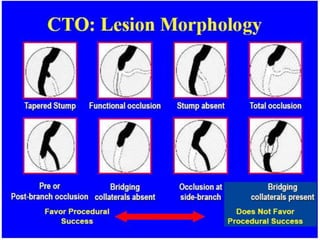
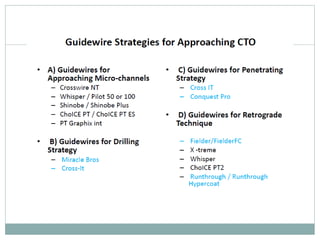
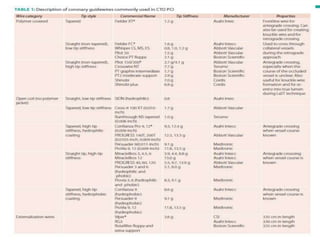
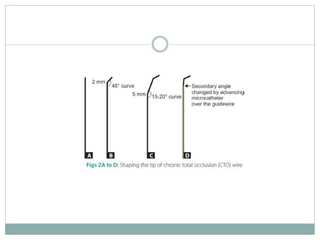
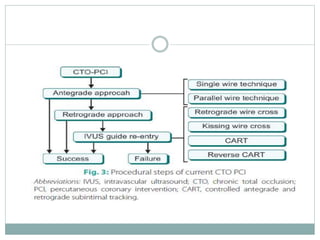
The document discusses strategies for percutaneous coronary intervention (PCI) of chronic total occlusions (CTOs). It describes:
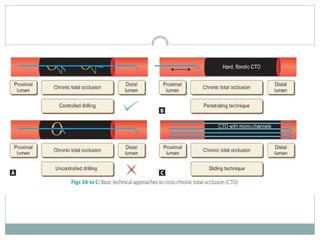
1. The antegrade approach is the most commonly used, with success rates of 60-80%. Tapered guidewires are first-choice to probe microchannels.
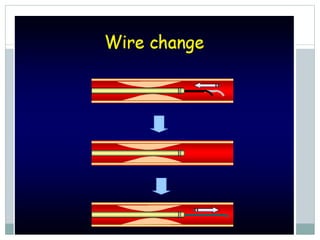
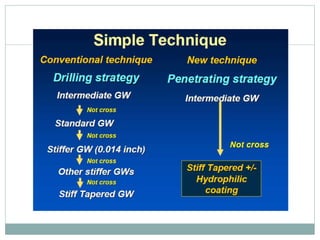
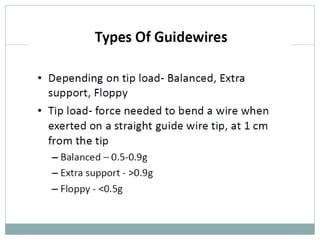
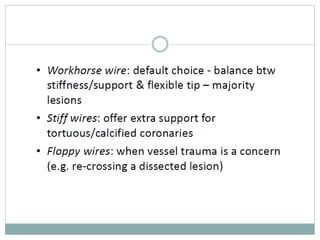
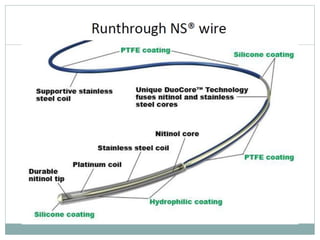
2. A four-wire strategy is recommended, starting with a polymer-coated wire and progressing to stiffer wires if needed.
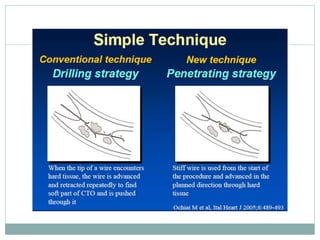
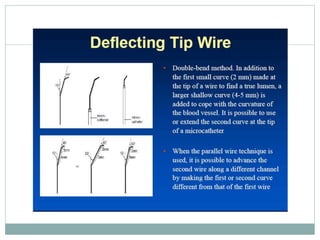
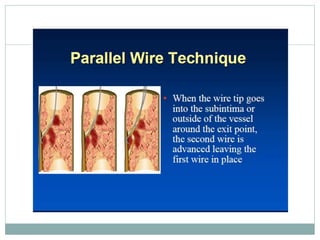
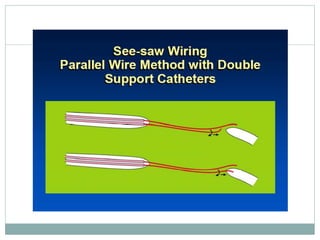
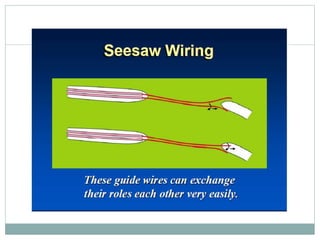
3. Advanced techniques like parallel wiring or antegrade dissection and reentry may be used if initial wiring fails.