Downloaded 23 times



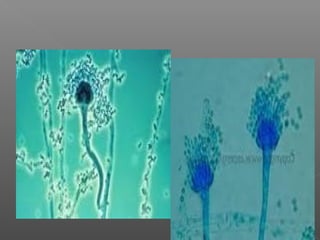

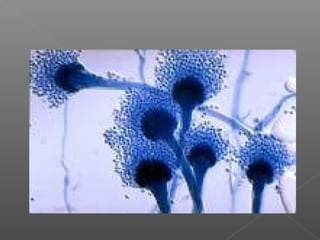





This document summarizes Aspergillus, a ubiquitous fungus with several species that can cause disease in humans. It describes the morphology and life cycle of Aspergillus, noting that its airborne conidia can reach the lungs and cause infection in immunocompromised individuals. It outlines the different clinical forms of aspergillosis, including allergic forms and risk factors. Diagnosis involves microscopy and culture of specimens. Treatment involves antifungal drugs like itraconazole and amphotericin B. Prevention focuses on avoiding exposure to conidia for at-risk groups.
































![[Int. med] cerebrovascular accident from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/hzgvfafesskr5a07k2so-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171704-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Gen. surg] tumours from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/hihk8xwqqeozwprtlpvo-signature-488639c0f2ed9772258765aac732a52dc3089a746e9bf5544a488c47cab4cc69-poli-150813092039-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Behv. sci] stress management by SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/cltz4ljwt3knztztzeem-signature-413e8c33574c21294a6dc95e37151f54f981375d6b0f4695b85074f597ea60c2-poli-150813085608-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)

![[Gen. surg] immunity and surgery from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/liqqmjo1qxwxerpux5hz-signature-488639c0f2ed9772258765aac732a52dc3089a746e9bf5544a488c47cab4cc69-poli-150813092038-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] pathogenesis](https://cdn.slidesharecdn.com/ss_thumbnails/reicxvotaytkxx8xnaam-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] chemical sterilizaton](https://cdn.slidesharecdn.com/ss_thumbnails/xwi6imyrrchg97geohxj-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)


![[Int. med] the sensory system from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/7xvc8ucgqb6ynpfpjojo-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] history taking from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/gkj8bezysaeqz6pg6qef-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171707-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial genetics (12 jan)](https://cdn.slidesharecdn.com/ss_thumbnails/ybiw66hrget4bdnxz447-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Pharma] receptors](https://cdn.slidesharecdn.com/ss_thumbnails/pharmareceptors-150502144616-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Behav. sci] psychosocial aspects of health by SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/94zxb2uqqni86crnqqer-signature-413e8c33574c21294a6dc95e37151f54f981375d6b0f4695b85074f597ea60c2-poli-150813085609-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] actinomyces](https://cdn.slidesharecdn.com/ss_thumbnails/9ecmrhoqrkocvbxkfudx-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] dyspnoea from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/abzzxuaq6syvtq38vxxq-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171657-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)




















![[Micro] syphilis](https://cdn.slidesharecdn.com/ss_thumbnails/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] sterilization](https://cdn.slidesharecdn.com/ss_thumbnails/jtli2uutrkcchg3xbjaw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] mycobacterium tuberculosis](https://cdn.slidesharecdn.com/ss_thumbnails/knwspassdmixhofx5ycy-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] parvovirus](https://cdn.slidesharecdn.com/ss_thumbnails/9efvufm6tsedx9o58t7q-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] hymenolepis nana](https://cdn.slidesharecdn.com/ss_thumbnails/3rxjz7ekrwinb1sq3uxs-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] gram positive spore bearing rods](https://cdn.slidesharecdn.com/ss_thumbnails/xi8ojr00samkfuo2qtsz-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] opportunistic mycosis](https://cdn.slidesharecdn.com/ss_thumbnails/r9htdghqrikznf5hrtly-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] mycobacterium leprae](https://cdn.slidesharecdn.com/ss_thumbnails/i6vamgi4rq2srkk4yof7-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] growth and culturing of bacteria](https://cdn.slidesharecdn.com/ss_thumbnails/xfkdsyhfs92guomky6hu-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] classification of prokaryotes](https://cdn.slidesharecdn.com/ss_thumbnails/6kp4xq4eqt6dbdni5yhj-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] clostridia](https://cdn.slidesharecdn.com/ss_thumbnails/rosblh0htbiwcq9fv3y4-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial genetics (6 jan)](https://cdn.slidesharecdn.com/ss_thumbnails/capdzkrqktd9kgwl1skw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial selective & differential media](https://cdn.slidesharecdn.com/ss_thumbnails/inykegaks3iuut4oc1pw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] cestodes](https://cdn.slidesharecdn.com/ss_thumbnails/nvpl1fbyq2ofjfsbmped-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] atypical mycobacterium](https://cdn.slidesharecdn.com/ss_thumbnails/7d5djanirg26boloifek-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] adenoviruses](https://cdn.slidesharecdn.com/ss_thumbnails/rqzzph7ktam2nsjysnxg-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

![[Int. med] approach to joint pain from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/064ftjyatacrqjgurlzo-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171713-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] anemia from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/8jbxzbhmt3ubllhnbjeg-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171706-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] chest pain 3rd year class from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/zkh5x8lztsickjayhfry-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171705-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)