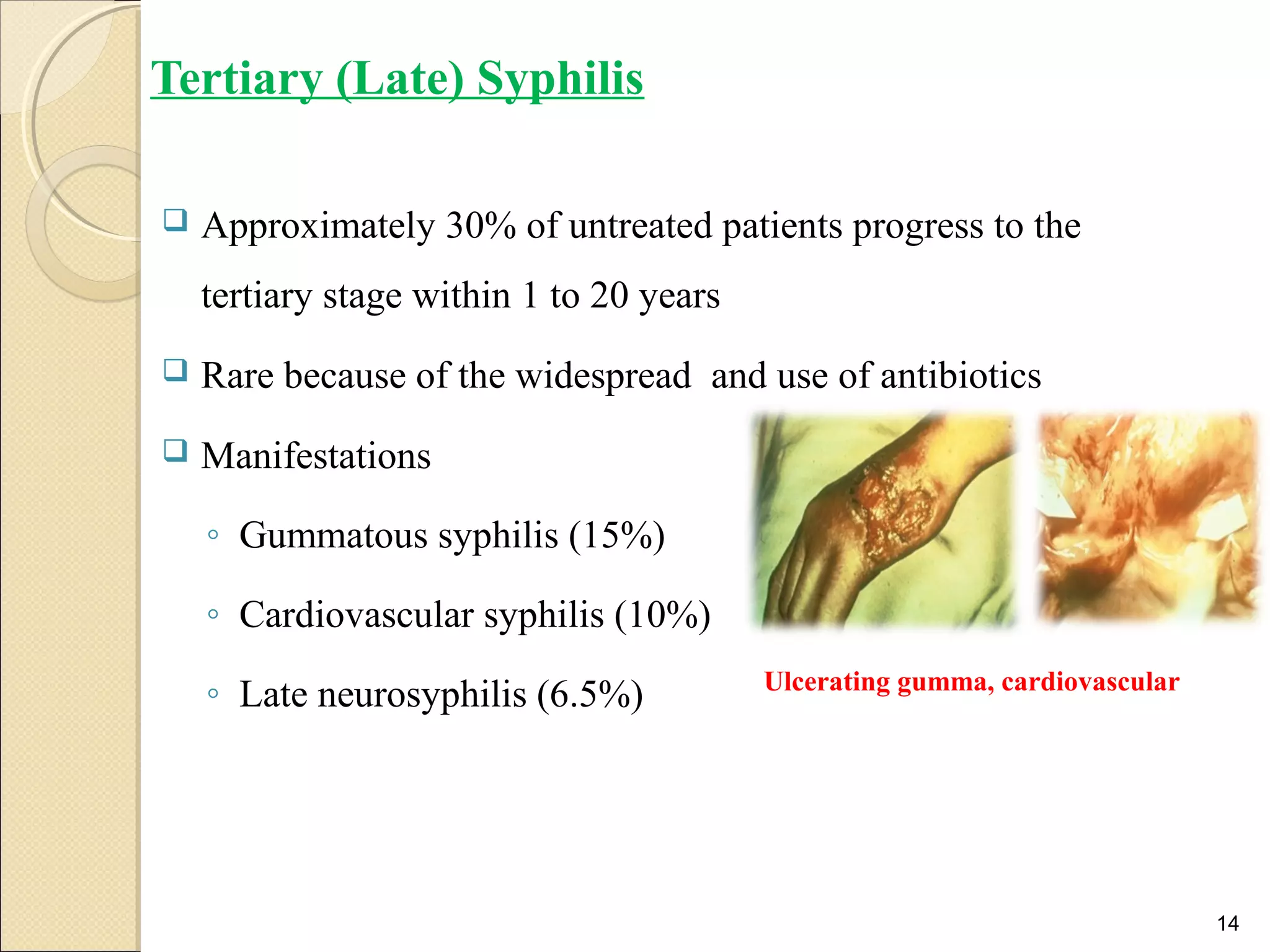
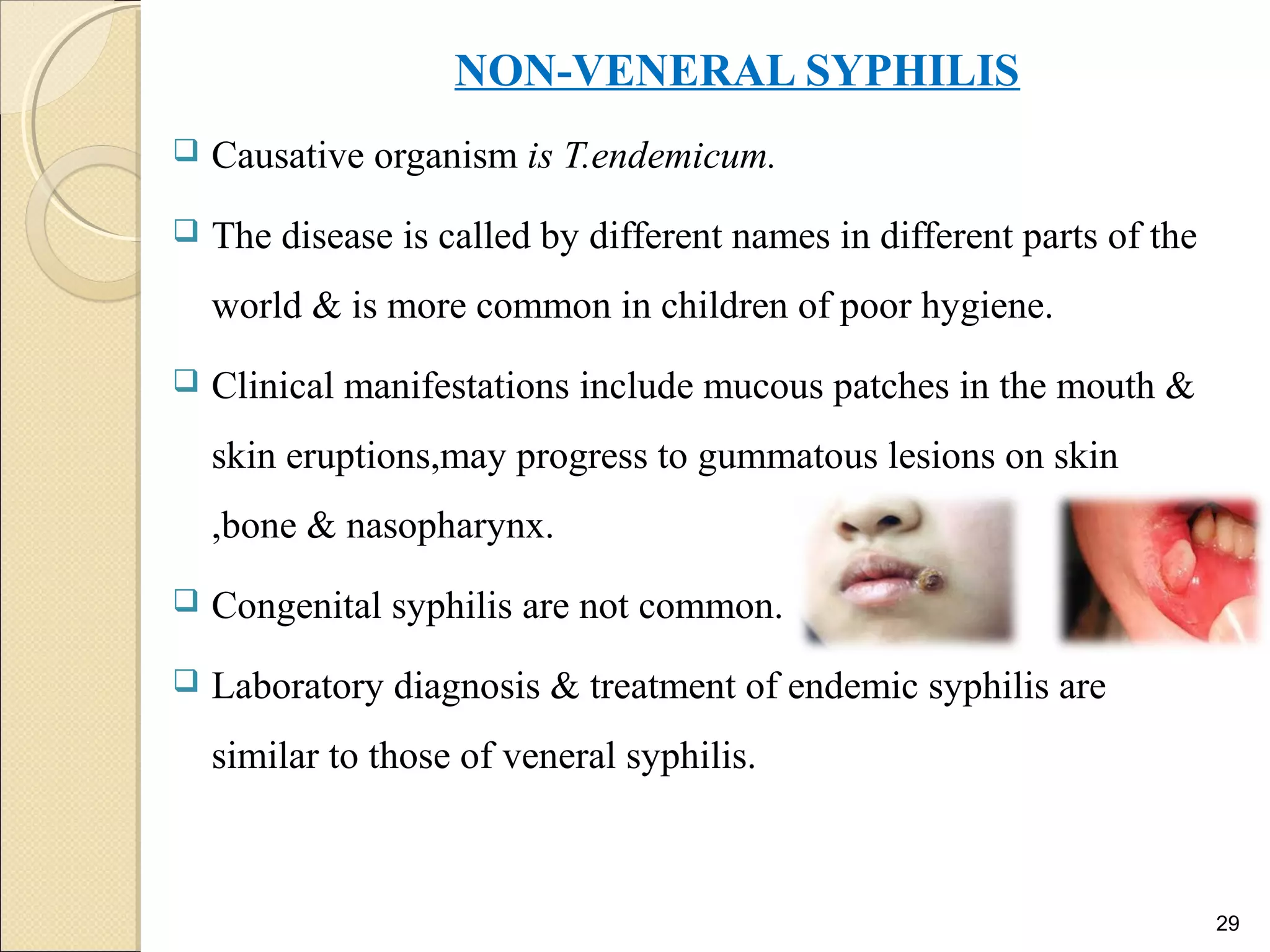
Syphilis is a sexually transmitted disease caused by the bacterium Treponema pallidum. It has four stages - primary, secondary, latent, and tertiary. The document provides an overview of the history, morphology, culture characteristics, epidemiology, pathogenesis, signs and symptoms, diagnostic tests, prophylaxis, and treatment for each stage of syphilis. Laboratory diagnosis involves darkfield microscopy, serological tests like VDRL and TPPA. Penicillin is usually used for treatment, while prevention involves condom use and testing of pregnant women.