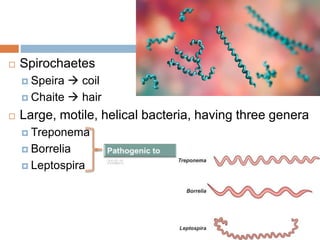
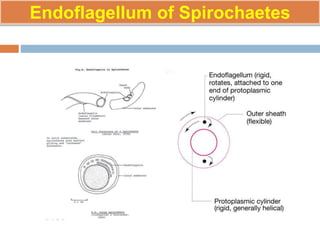

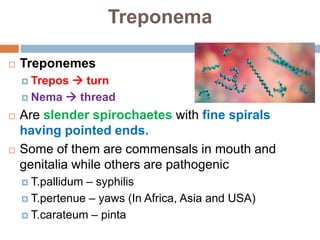
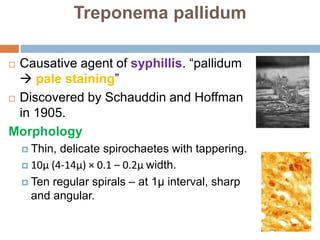
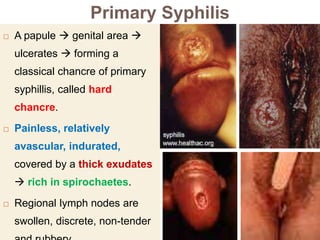
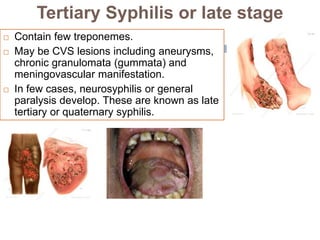
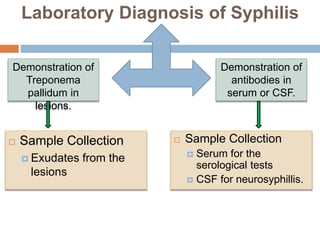
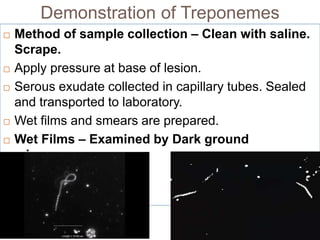



Spirochaetes are helical bacteria that possess endoflagella between their outer membrane and cell wall. This allows them to move via flexing, rotation, or translation. Treponema pallidum is the spirochete that causes syphilis. It has a multi-stage lifecycle going from primary chancre lesions, to disseminated secondary lesions, and potentially late-stage tertiary lesions affecting organs. Diagnosis involves direct visualization of T. pallidum in lesions or serological tests detecting antibodies against cardiolipin or treponemal antigens.


















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




