Downloaded 489 times

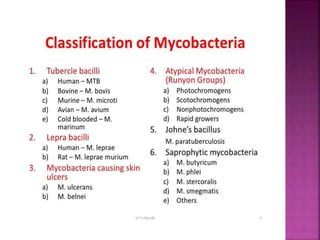
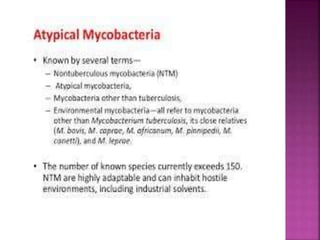
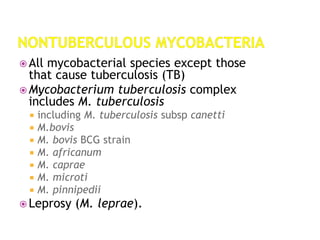
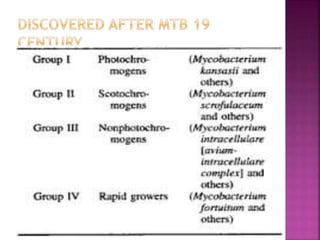
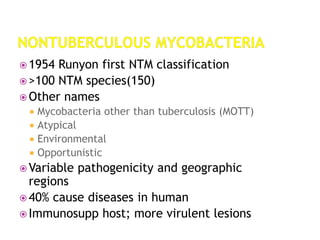
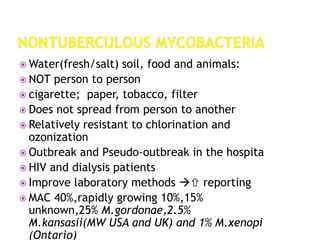
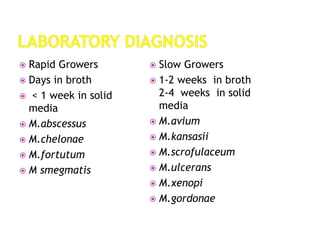

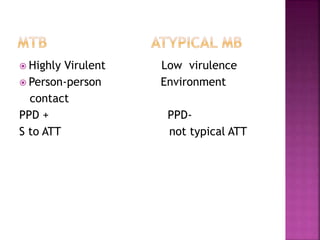
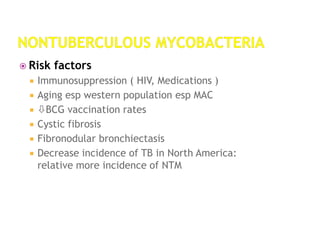
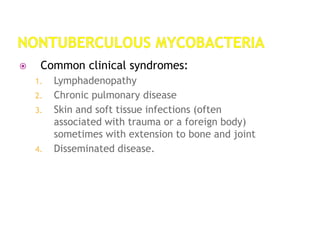
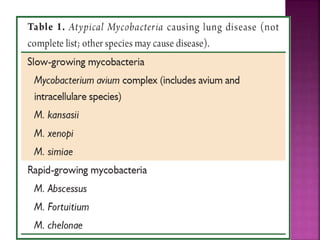

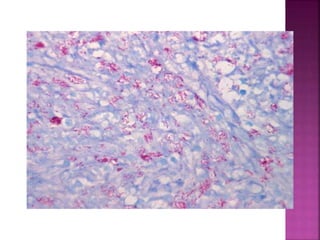




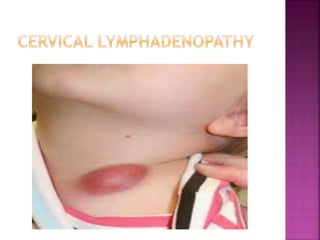



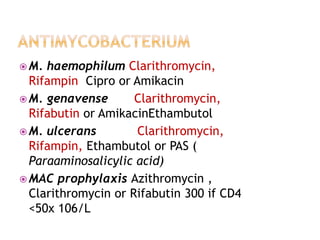

Non-tuberculous mycobacteria (NTM) include all mycobacterial species except those in the Mycobacterium tuberculosis complex which cause tuberculosis. There are over 150 identified NTM species, some of which can cause disease in humans, especially in immunosuppressed individuals. NTM are commonly found in the environment including water and soil. Common diseases caused by NTM include pulmonary disease, lymphadenitis, and skin and soft tissue infections. Treatment involves a combination of antimicrobials and is based on the species isolated and results of drug susceptibility testing.

























































![mikrobiyoloji_6._ders_son[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/mikrobiyoloji6-231012150214-35c792ed-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] syphilis](https://cdn.slidesharecdn.com/ss_thumbnails/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] sterilization](https://cdn.slidesharecdn.com/ss_thumbnails/jtli2uutrkcchg3xbjaw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] mycobacterium tuberculosis](https://cdn.slidesharecdn.com/ss_thumbnails/knwspassdmixhofx5ycy-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] pathogenesis](https://cdn.slidesharecdn.com/ss_thumbnails/reicxvotaytkxx8xnaam-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] parvovirus](https://cdn.slidesharecdn.com/ss_thumbnails/9efvufm6tsedx9o58t7q-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] hymenolepis nana](https://cdn.slidesharecdn.com/ss_thumbnails/3rxjz7ekrwinb1sq3uxs-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] gram positive spore bearing rods](https://cdn.slidesharecdn.com/ss_thumbnails/xi8ojr00samkfuo2qtsz-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] opportunistic mycosis](https://cdn.slidesharecdn.com/ss_thumbnails/r9htdghqrikznf5hrtly-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] mycobacterium leprae](https://cdn.slidesharecdn.com/ss_thumbnails/i6vamgi4rq2srkk4yof7-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] aspergillus](https://cdn.slidesharecdn.com/ss_thumbnails/f74upwejq4u9rqvunxal-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] growth and culturing of bacteria](https://cdn.slidesharecdn.com/ss_thumbnails/xfkdsyhfs92guomky6hu-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] chemical sterilizaton](https://cdn.slidesharecdn.com/ss_thumbnails/xwi6imyrrchg97geohxj-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] classification of prokaryotes](https://cdn.slidesharecdn.com/ss_thumbnails/6kp4xq4eqt6dbdni5yhj-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] clostridia](https://cdn.slidesharecdn.com/ss_thumbnails/rosblh0htbiwcq9fv3y4-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190754-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial genetics (6 jan)](https://cdn.slidesharecdn.com/ss_thumbnails/capdzkrqktd9kgwl1skw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial selective & differential media](https://cdn.slidesharecdn.com/ss_thumbnails/inykegaks3iuut4oc1pw-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] cestodes](https://cdn.slidesharecdn.com/ss_thumbnails/nvpl1fbyq2ofjfsbmped-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] bacterial genetics (12 jan)](https://cdn.slidesharecdn.com/ss_thumbnails/ybiw66hrget4bdnxz447-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] adenoviruses](https://cdn.slidesharecdn.com/ss_thumbnails/rqzzph7ktam2nsjysnxg-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Micro] actinomyces](https://cdn.slidesharecdn.com/ss_thumbnails/9ecmrhoqrkocvbxkfudx-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190753-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)