This document provides information about the bacteria Spirochaetes. It discusses their morphology, motility, reproduction, pathogenic species, diseases caused, and laboratory diagnosis. Some key points:
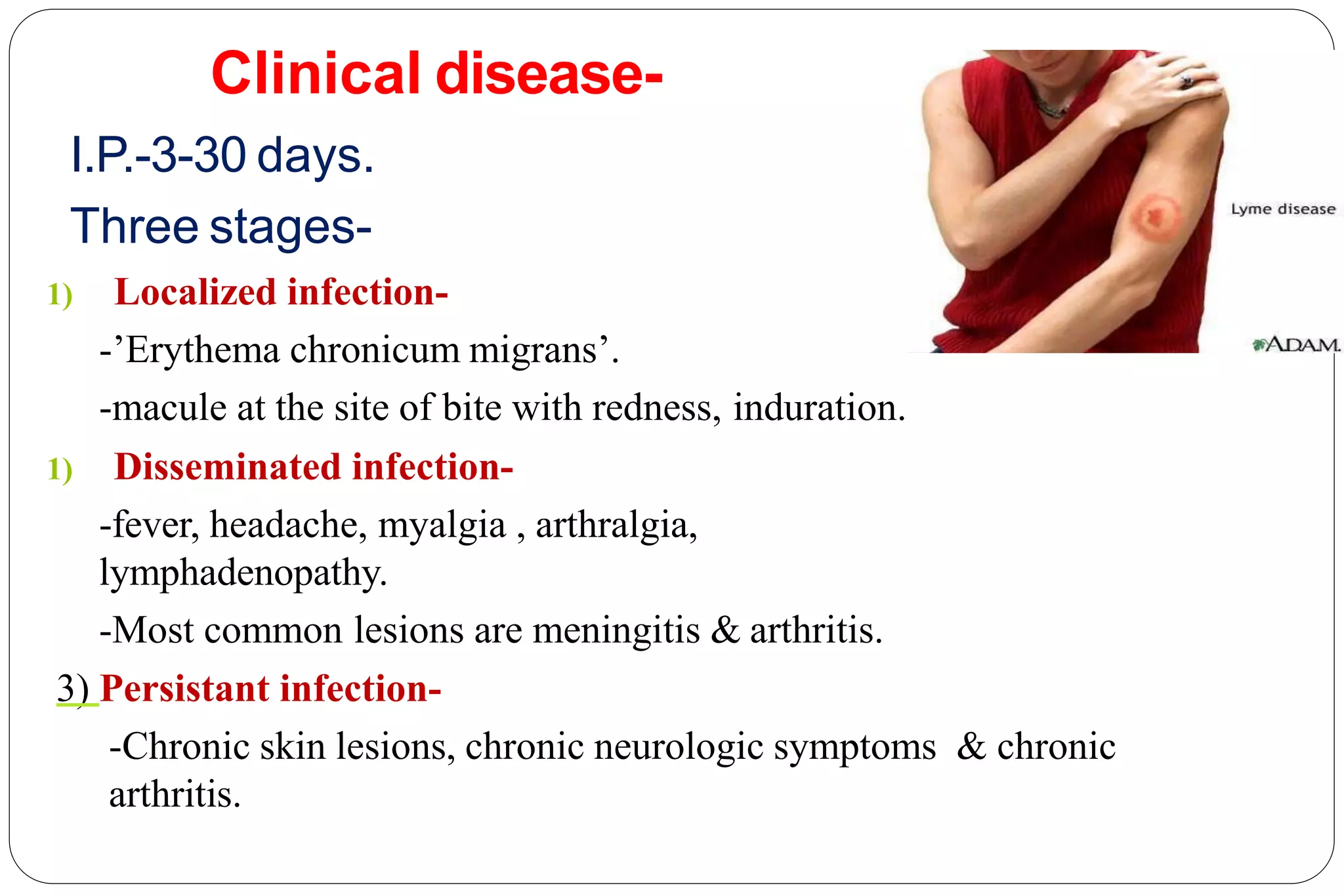
- Spirochaetes are elongated, helically coiled, and motile bacteria with endoflagella. They can cause diseases like syphilis, Lyme disease, and leptospirosis.
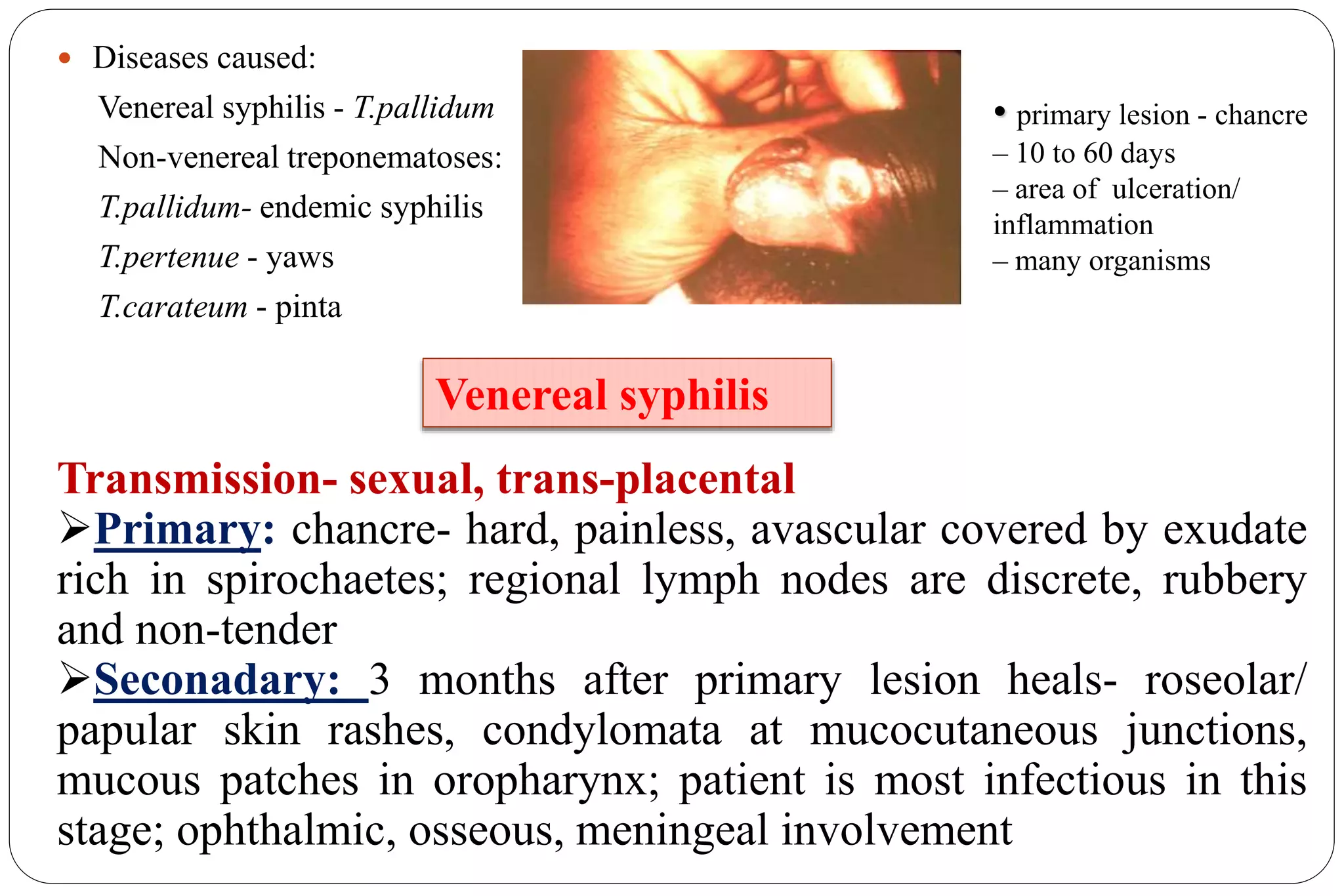
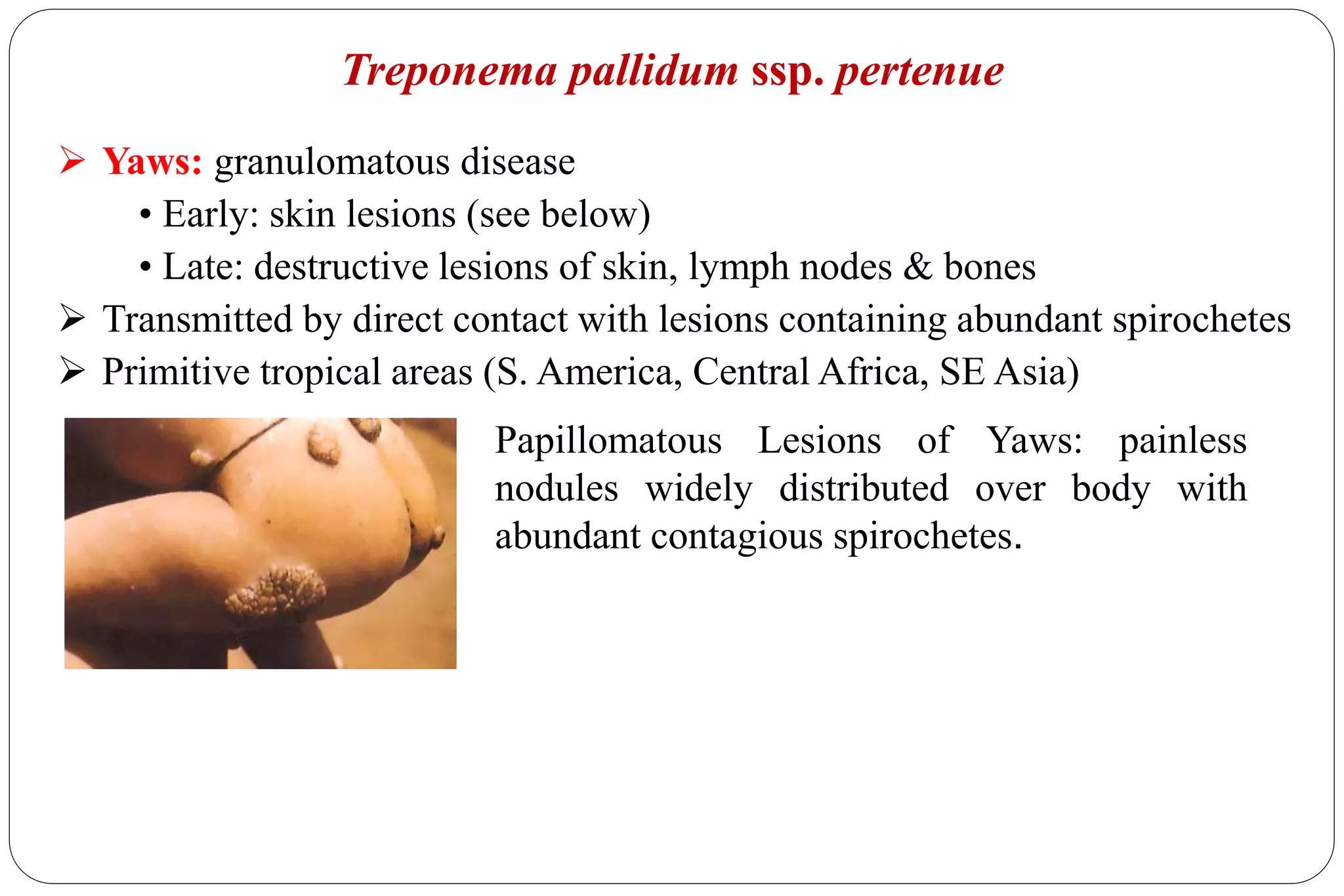
- Pathogenic species include Treponema pallidum (syphilis), Borrelia burgdorferi (Lyme disease), and Leptospira interrogans (leptospirosis).
- Laboratory diagnosis involves darkfield microscopy, culture, serology, and







































































![[Micro] syphilis](https://cdn.slidesharecdn.com/ss_thumbnails/loot4qpwrfcwmtl9jo3e-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)






































