Downloaded 177 times
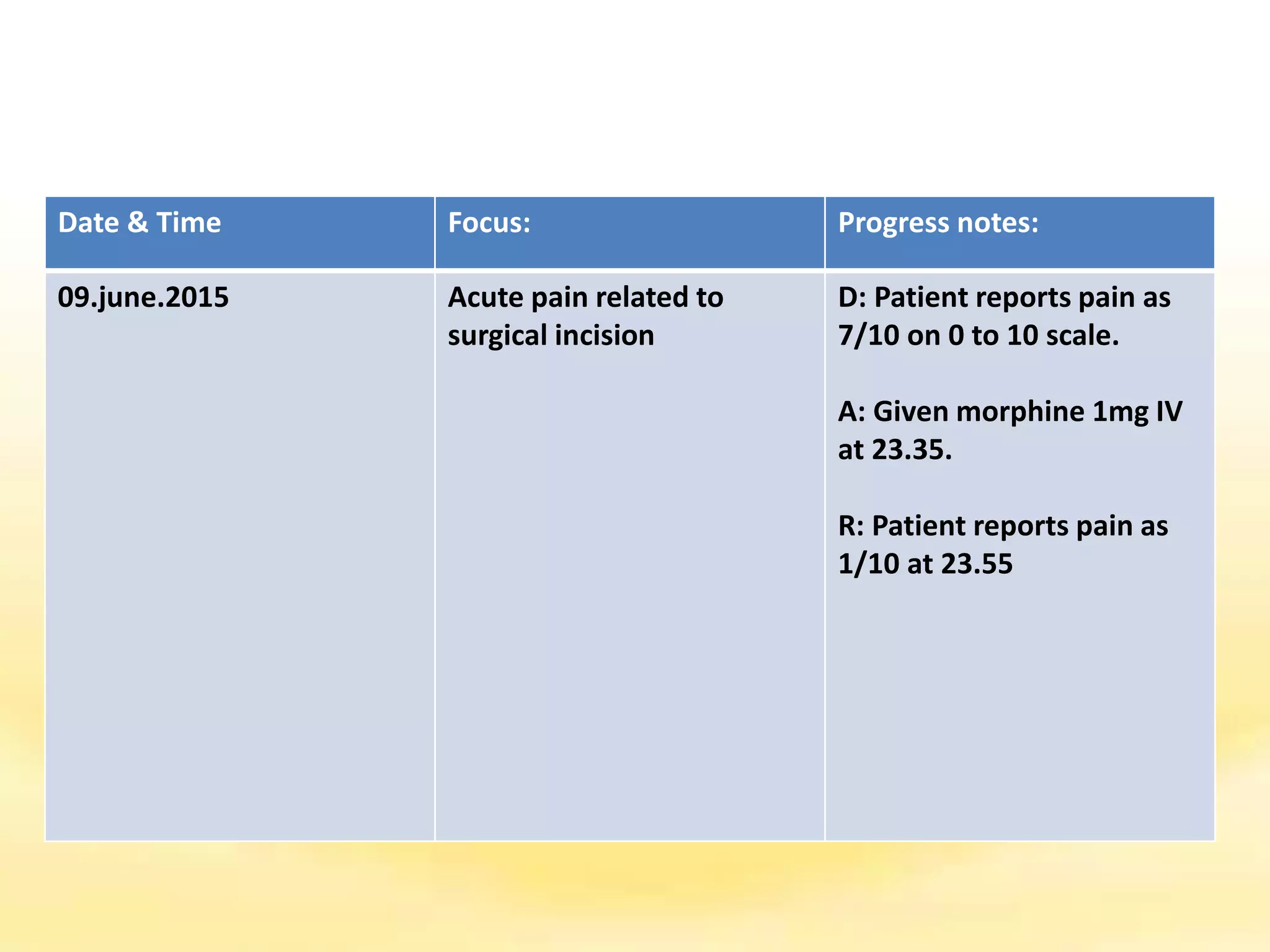


There are several documentation systems used in healthcare to record patient data, either electronically or on paper. Some common systems include narrative charting, source-oriented charting, problem-oriented charting using the SOAP format, PIE charting, focus charting, charting by exception, computerized documentation, and case management using critical paths. Problem-oriented charting using the SOAP format is a structured approach that documents subjective data, objective data, assessment, and plan.




















































![[1] documentation and reporting](https://cdn.slidesharecdn.com/ss_thumbnails/1documentationandreporting-150205213856-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)