



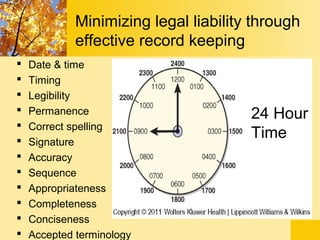

The document discusses documentation and reporting in healthcare. It defines documentation as a permanent record of client information and care. Documentation serves several purposes such as communication between providers, legal documentation, research, and education. The document outlines various methods of documentation including narrative charting, problem-oriented charting, and computerized documentation. It also discusses different types of records like the kardex, flow sheets, and discharge summary used for recording client data. Verbal reporting is also an important communication technique in healthcare.










































![[1] documentation and reporting](https://cdn.slidesharecdn.com/ss_thumbnails/1documentationandreporting-150205213856-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)