
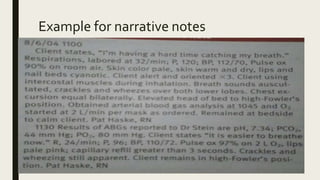




The document discusses various methods of nursing documentation and recording. It describes the purposes of accurate nursing documentation as communication, legal documentation, nursing audits, education, financial billing, nursing research, and improving the quality of care. The principles of quality documentation include being factual, accurate, complete, current, organized and timely. Common documentation methods discussed are narrative notes, problem-oriented medical records (POMR), source records, charting by exception, and case management plans.