Downloaded 90 times








































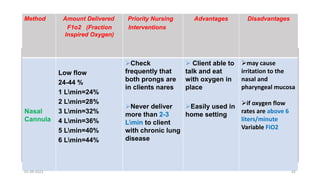











































































































The document discusses various factors that can affect a person's oxygenation needs. It describes several conditions that can affect the airway, including allergies, asthma, common colds, and bronchitis. It also discusses factors like dyspnea, tachypnea, and bradypnea that can affect breathing movements. Conditions like pulmonary edema, COPD, and atelectasis are mentioned as things that can impact gas diffusion in the lungs. Heart failure is provided as an example of something that can affect oxygen transport. The document concludes by covering nursing interventions for oxygen administration like various devices and their purposes, methods, and considerations.

























![Bandages and Binders [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bandagesandbindersautosaved-230314063514-38348509-thumbnail.jpg?width=640&height=640&fit=bounds)




























































