





























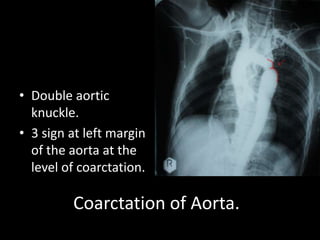


![• Dilated right
pulmonary artery.
• Right ventricular
enlargement :
– Acute angle.
– Apex shifted
outward.
• Prominent upper
lobe veins.
[Cephalization]
Mitral Valve Disease.](https://image.slidesharecdn.com/xrays-130131232343-phpapp01/85/Medicine-Xrays-42-320.jpg)










1. Chest x-ray showed free gas under the right hemidiaphragm. 2. This finding suggests a hiatal hernia, where part of the stomach protrudes through the diaphragm into the chest. 3. The 67-year old patient presented with chronic cough and mild heartburn, consistent with symptoms of a hiatal hernia.





































































































