![CARDIO-THORACIC RATIO
• (CR+CL)<(T/2)
• Normal Cardio-Thoracic ratio is less than 0.5 in adults [(CR+CL)/CT<0.5]
T](https://image.slidesharecdn.com/reading-chest-x-rays2-200515185051/85/Reading-chest-x-rays-27-320.jpg)





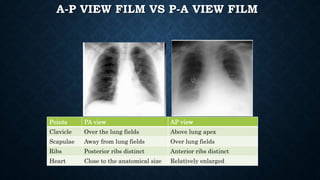
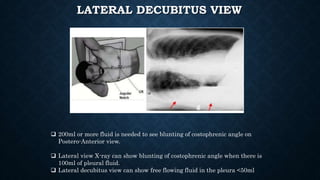
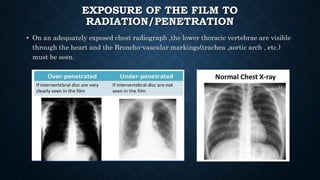
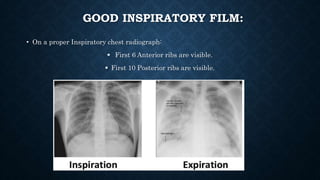
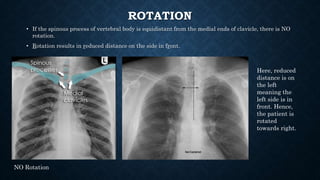
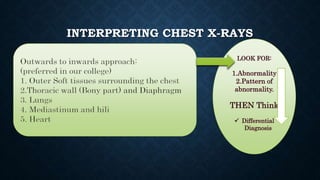
This document provides information on reading and interpreting chest x-rays. It begins with background on x-rays and radiographic densities seen on chest films. It describes the important details to note before interpreting a chest x-ray, including patient information, view, exposure, and breath status. The four main views of chest x-rays are described. Key structures seen on chest films are outlined, including the heart, diaphragm, lungs, and interfaces. Common abnormalities like pleural effusions, pneumothorax, and cardiomegaly are discussed. The document provides a thorough guide to evaluating all aspects of the chest on x-ray films.



































































