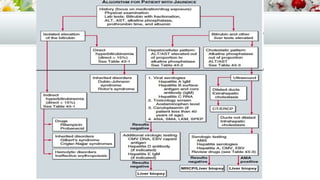
This document provides an overview of approaches to evaluating and diagnosing jaundice. It discusses the production and metabolism of bilirubin, measurement of bilirubin levels, clinical history and examination of patients, and laboratory and imaging tests used to classify jaundice as pre-hepatic, hepatocellular, or cholestatic. Common etiologies of each type are outlined, including inherited and acquired conditions.