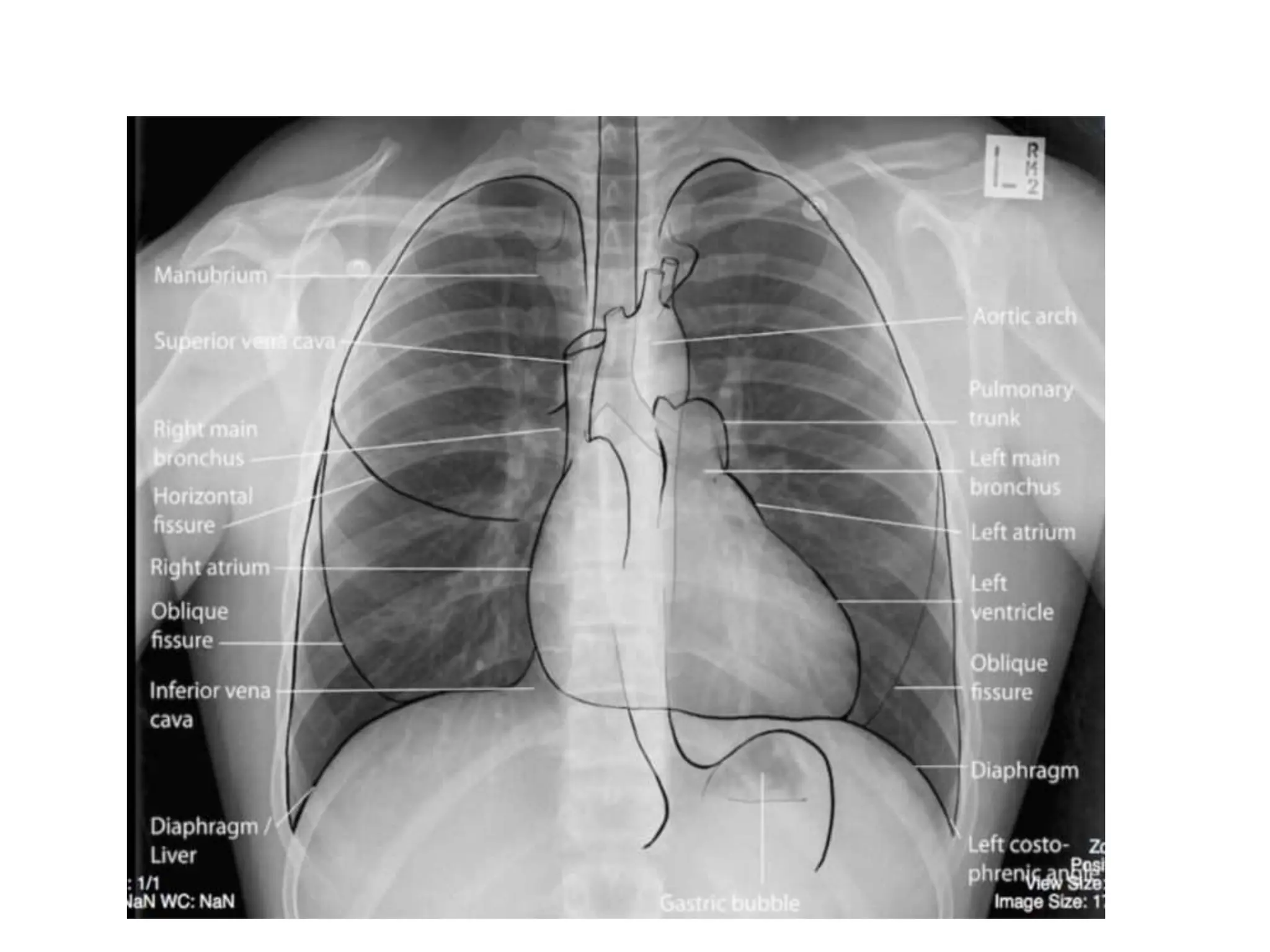
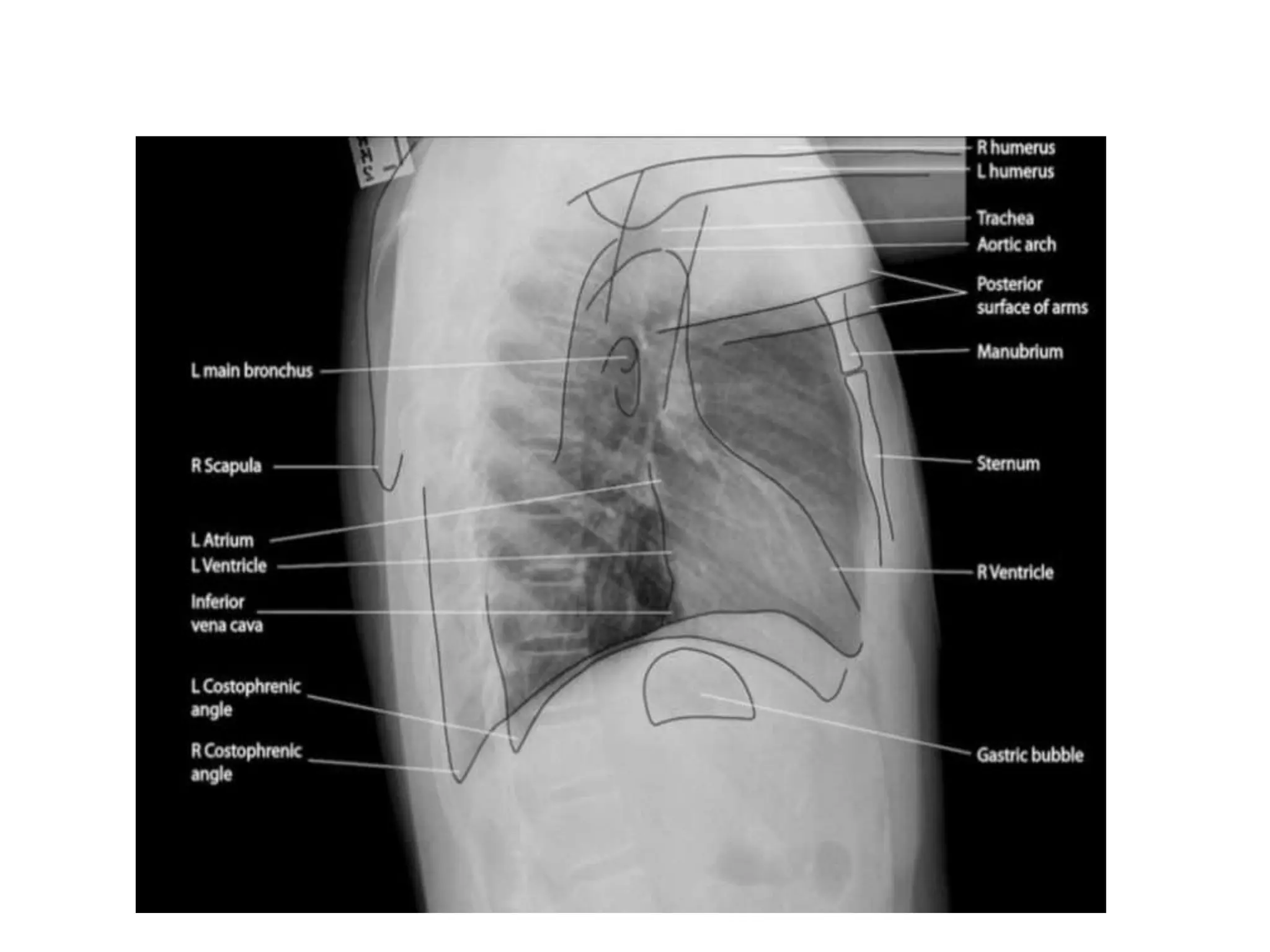
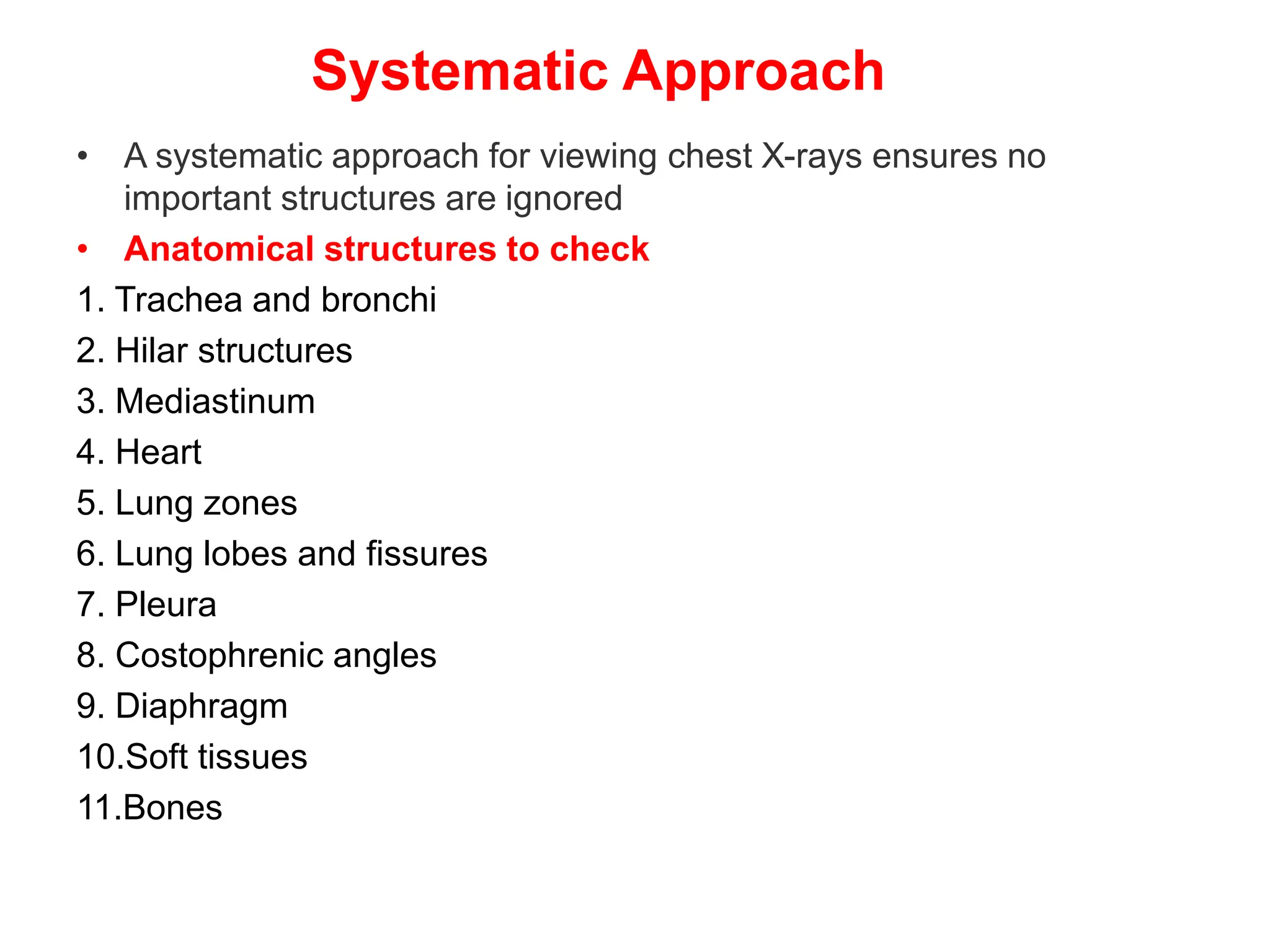
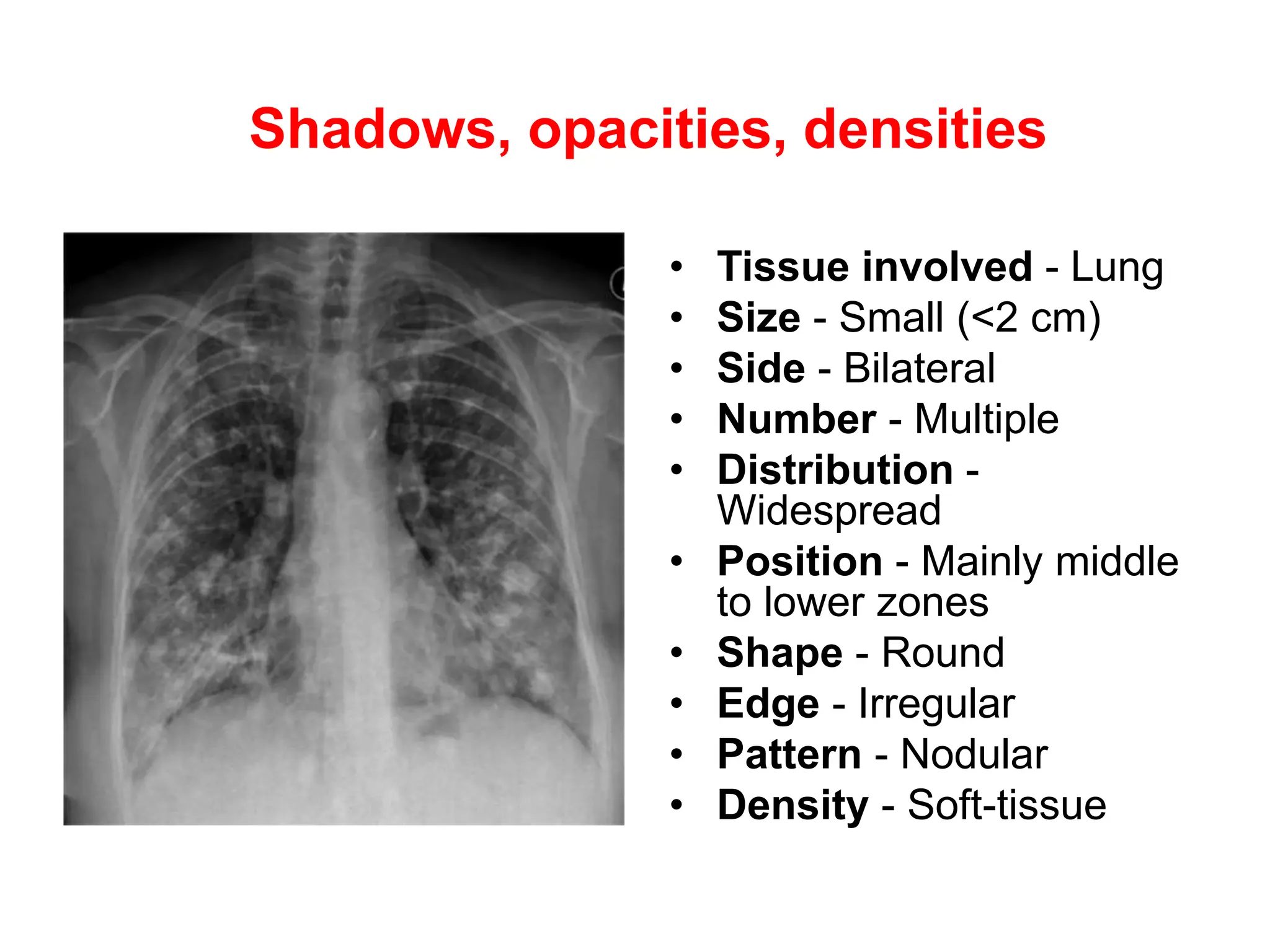
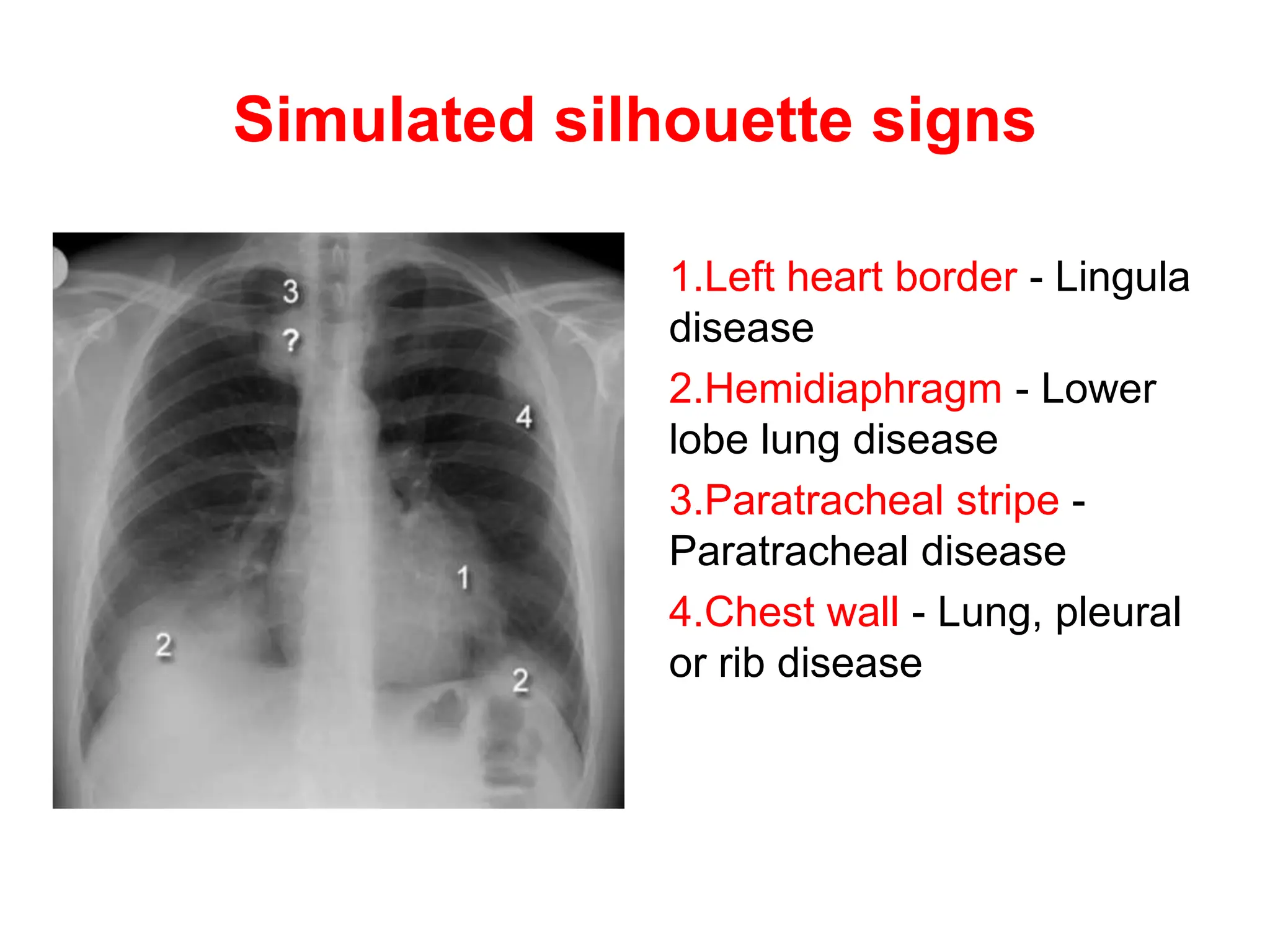
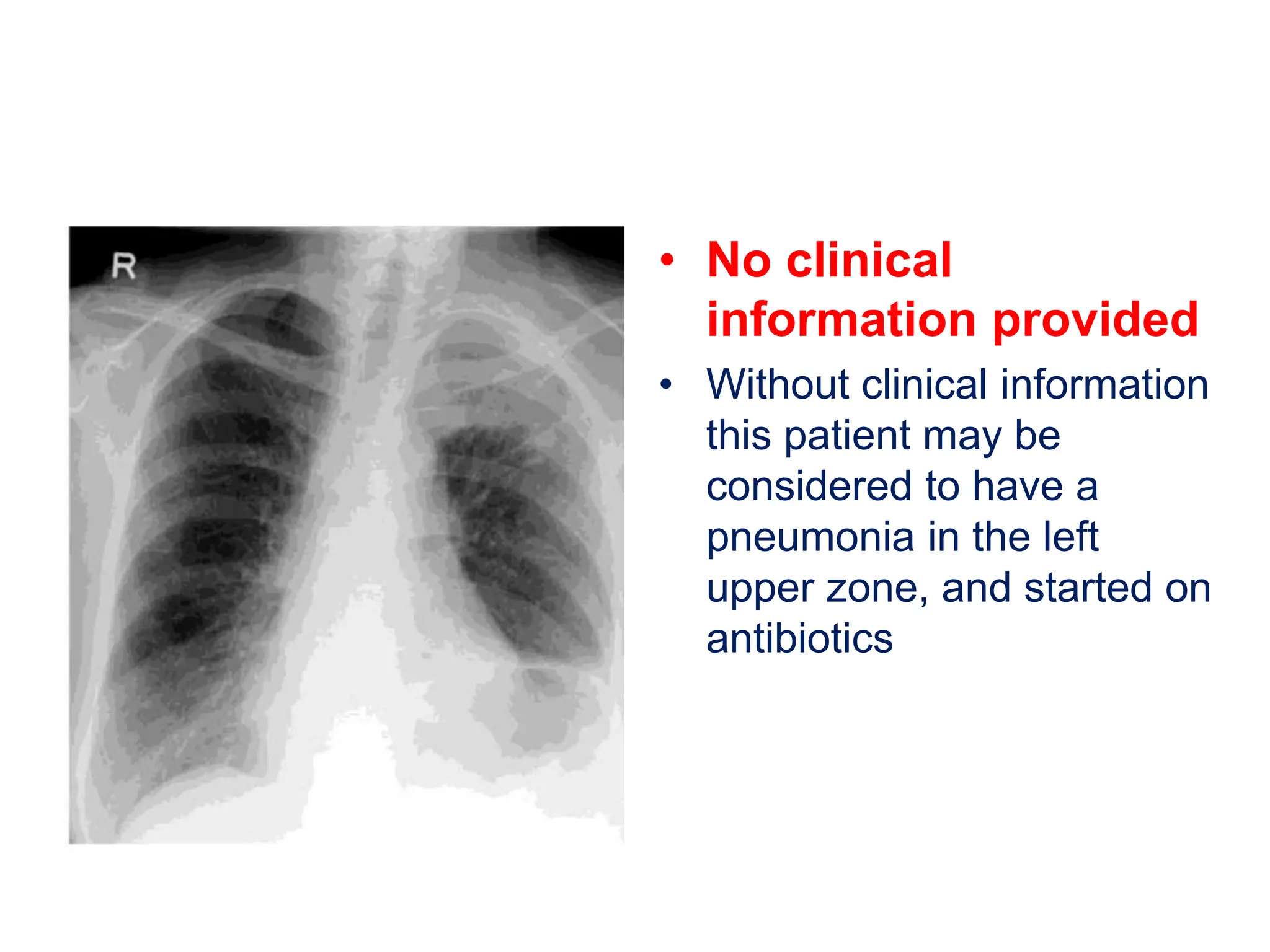
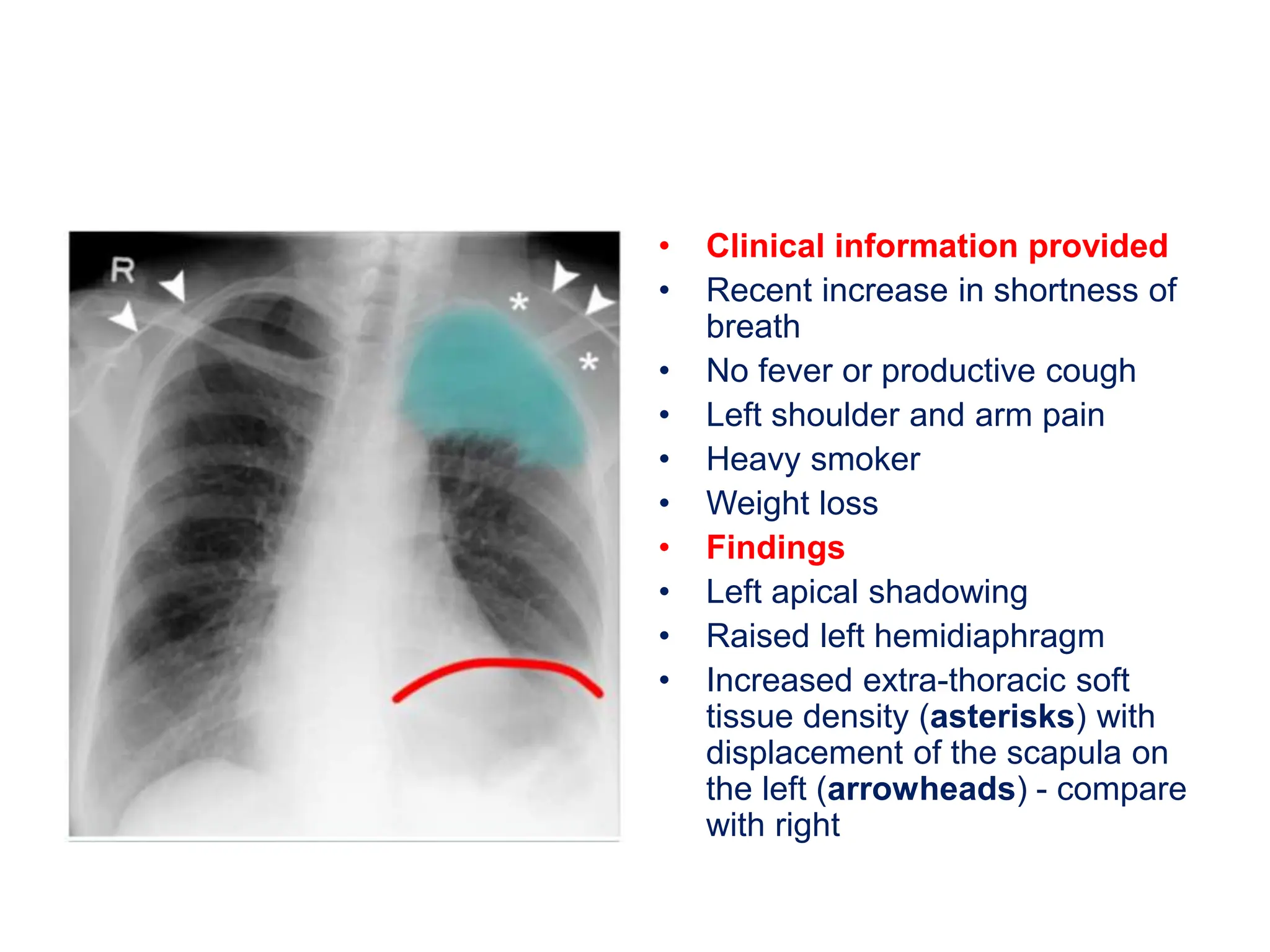
The document outlines a systematic approach for analyzing chest X-rays, emphasizing the review of anatomical structures and image quality as well as methods for describing and locating abnormalities. Key concepts include the silhouette sign, simulated silhouette signs, and the importance of considering clinical context when interpreting X-rays. Overall, the aim is to ensure a thorough examination to avoid missing significant pathologies.