Downloaded 1,770 times




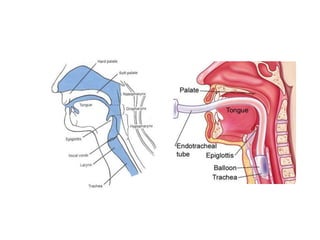
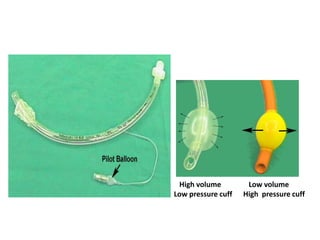


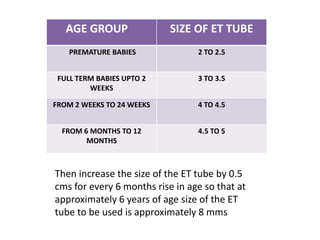







The document describes the components and uses of endotracheal tubes, which are curved plastic or latex tubes used for intubation to provide an airway for mechanical ventilation or respiratory support. It details the parts of the ET tube including the proximal end, central portion with markers, and distal end, as well as types, sizing, complications, and uses. The document also provides information on ambu bags, including their parts and mechanism for providing intermittent positive pressure ventilation.



































































