Downloaded 2,589 times
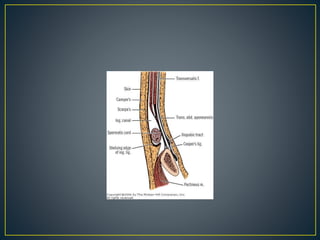
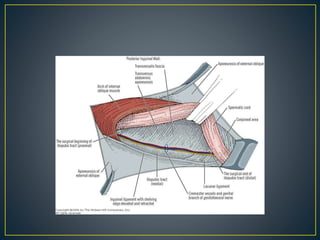
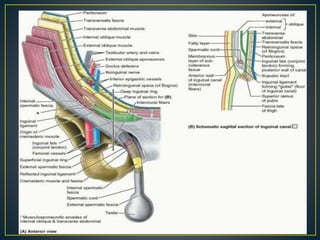

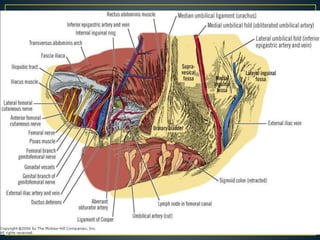

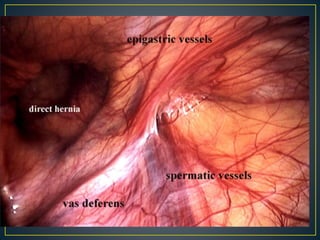
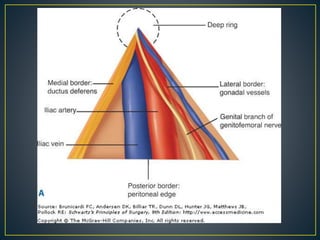
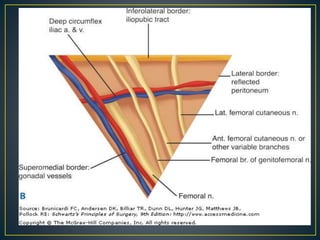
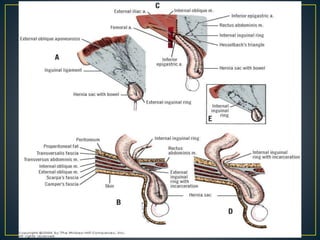
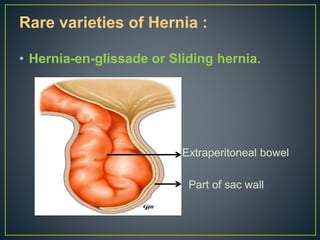
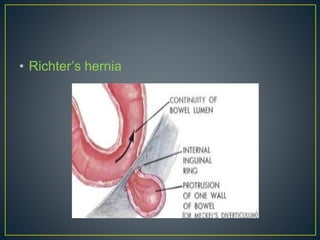

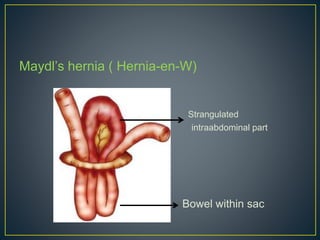
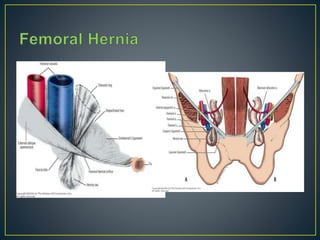
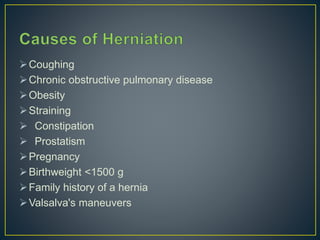
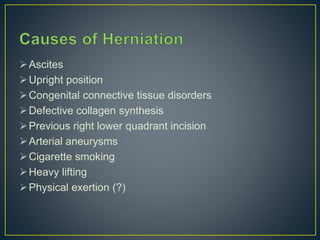
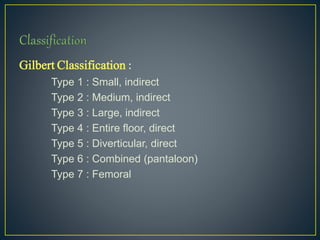

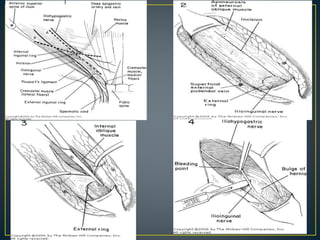
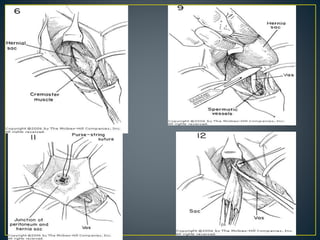
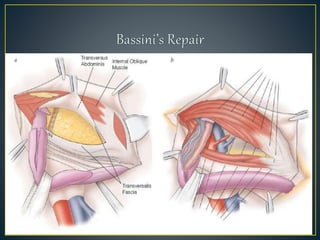
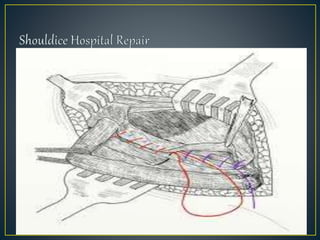
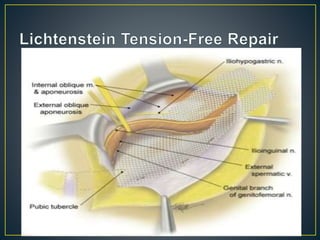

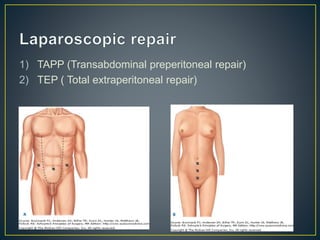
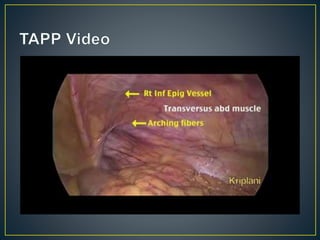


This document discusses hernias, including their anatomy, types, causes, diagnosis, and treatment options. It provides details on the layers of the abdominal wall and inguinal canal. There are two main types of hernias - indirect and direct. Treatment options include open repair techniques like Shouldice repair as well as laparoscopic techniques like TAPP and TEP which involve placing a mesh to reinforce the abdominal wall. Complications of hernia repair can include recurrence, chronic pain, infection, and injury to surrounding structures.
































































































