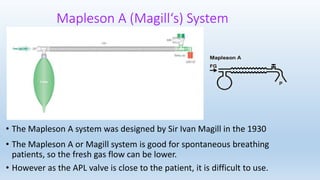
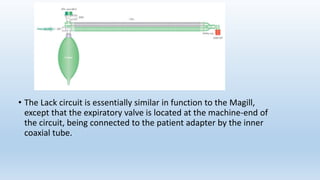
The document describes several Mapleson breathing systems used in anesthesia. It provides details on the Mapleson A, B, C, D systems as well as modifications like the Mapleson A-Lack system and the Bain circuit. The Bain circuit is highlighted as having advantages over other systems like being lightweight, causing minimal drag on the endotracheal tube, having low resistance, allowing for visualization of the inner tube, and facilitating both spontaneous and controlled ventilation with easier changeover between the two.