This document discusses anesthesia circuits, covering their definition, history, functions, classifications, and components. It details various types of circuits such as Mapleson A to F, their advantages, disadvantages, and methods for circuit integrity checks. The document also highlights the importance of effective gas delivery, CO2 elimination, and maintaining the patient's warmth and humidity during anesthesia.

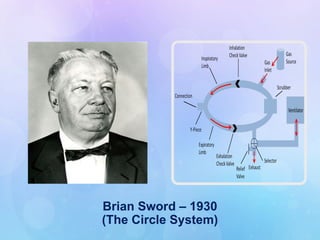


![CIRCLE SYSTEM
The Circle system can be either:
o Closed:- Fresh gas inflow exactly equal to patient
uptake, complete rebreathing after carbon dioxide
absorbed, and APL closed.
o Semi-closed :- Some rebreathing occurs, FGF and APL
settings at intermediate values .
o Semi-open :- No rebreathing, high fresh gas flow
[higher than minute ventilation].](https://image.slidesharecdn.com/circuitshemiii-241107153037-16809a67/85/Anaesthesia-Breathing-Circuits-ppt-Hemant-48-320.jpg)