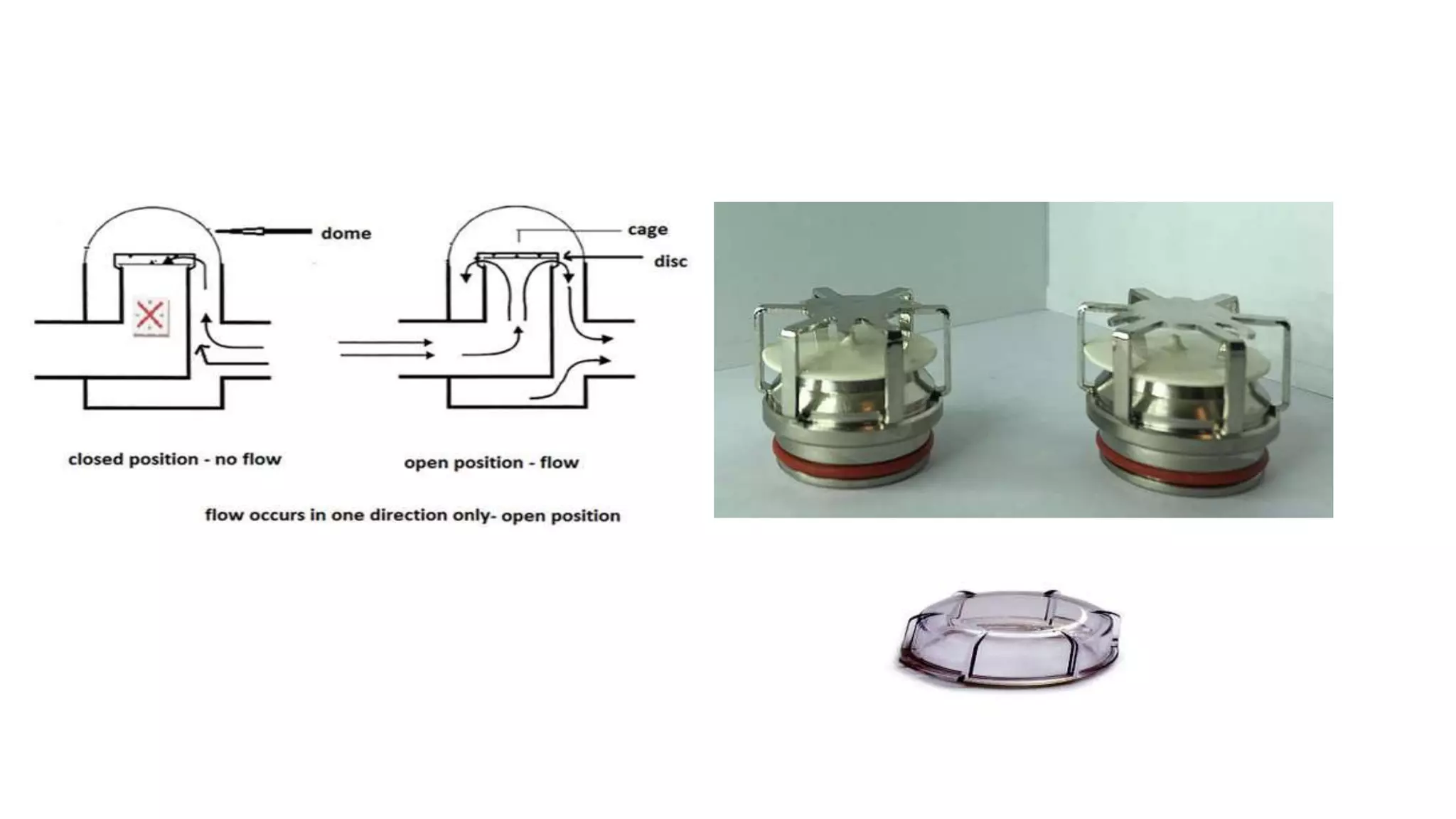
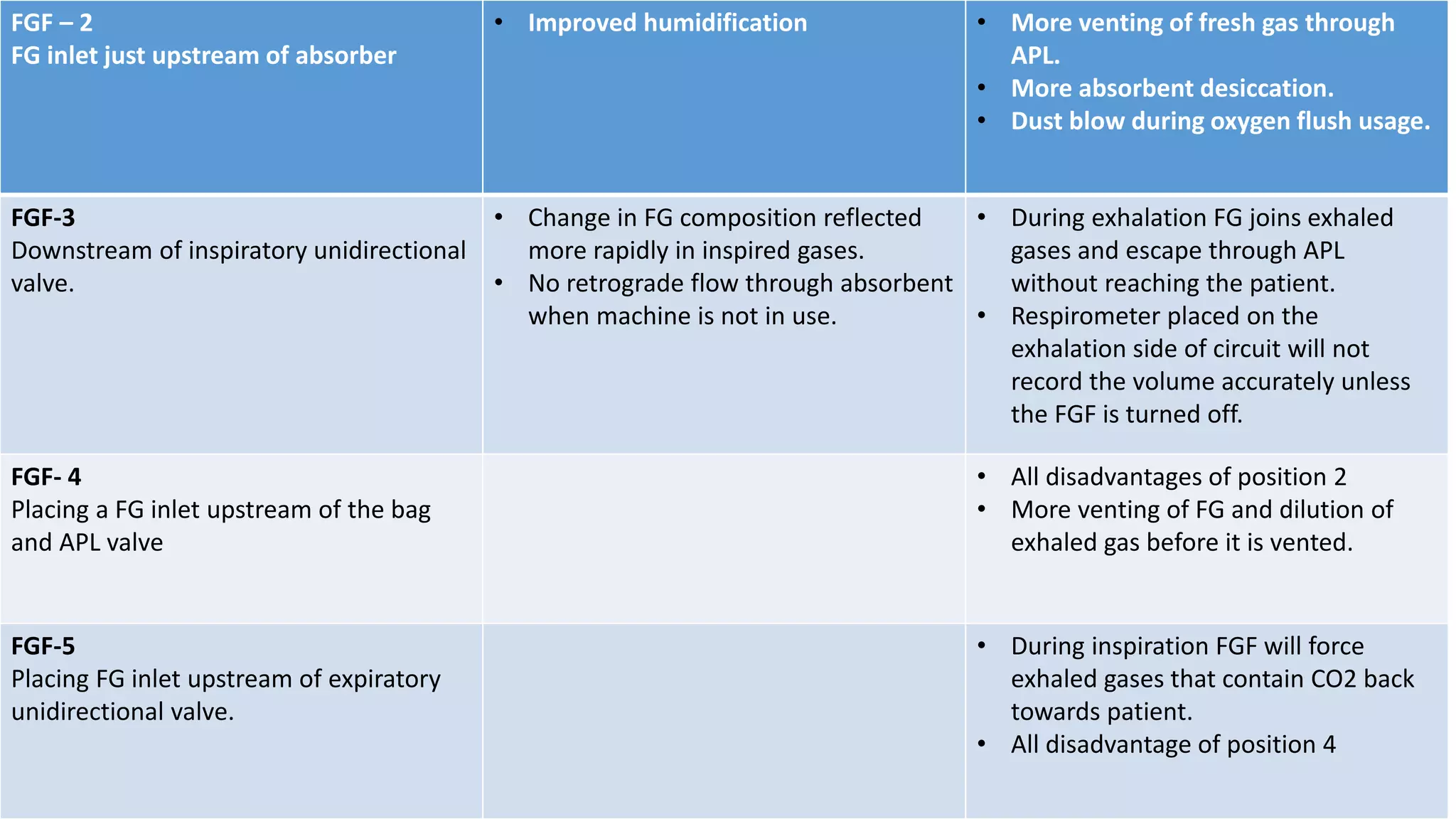
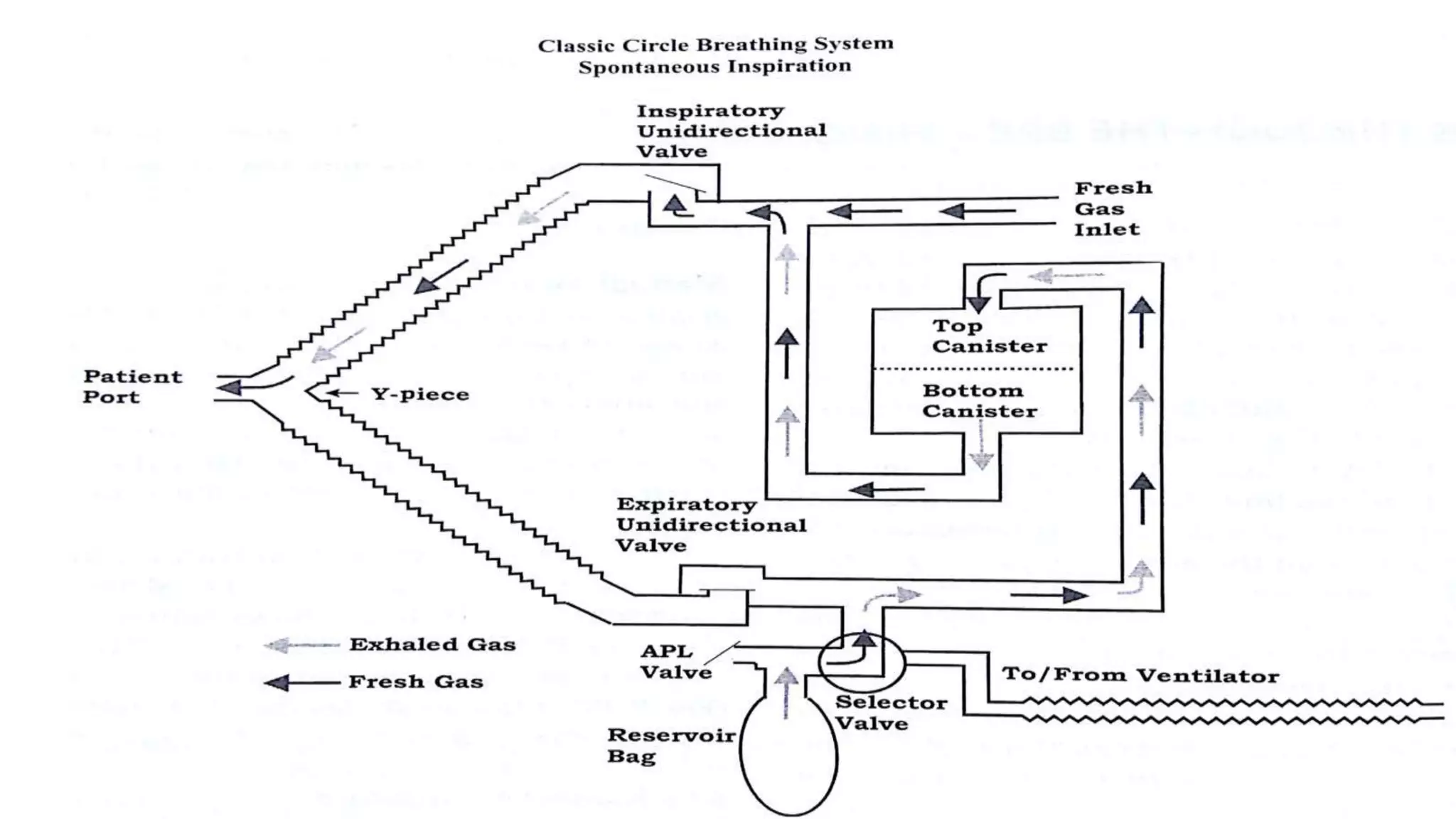
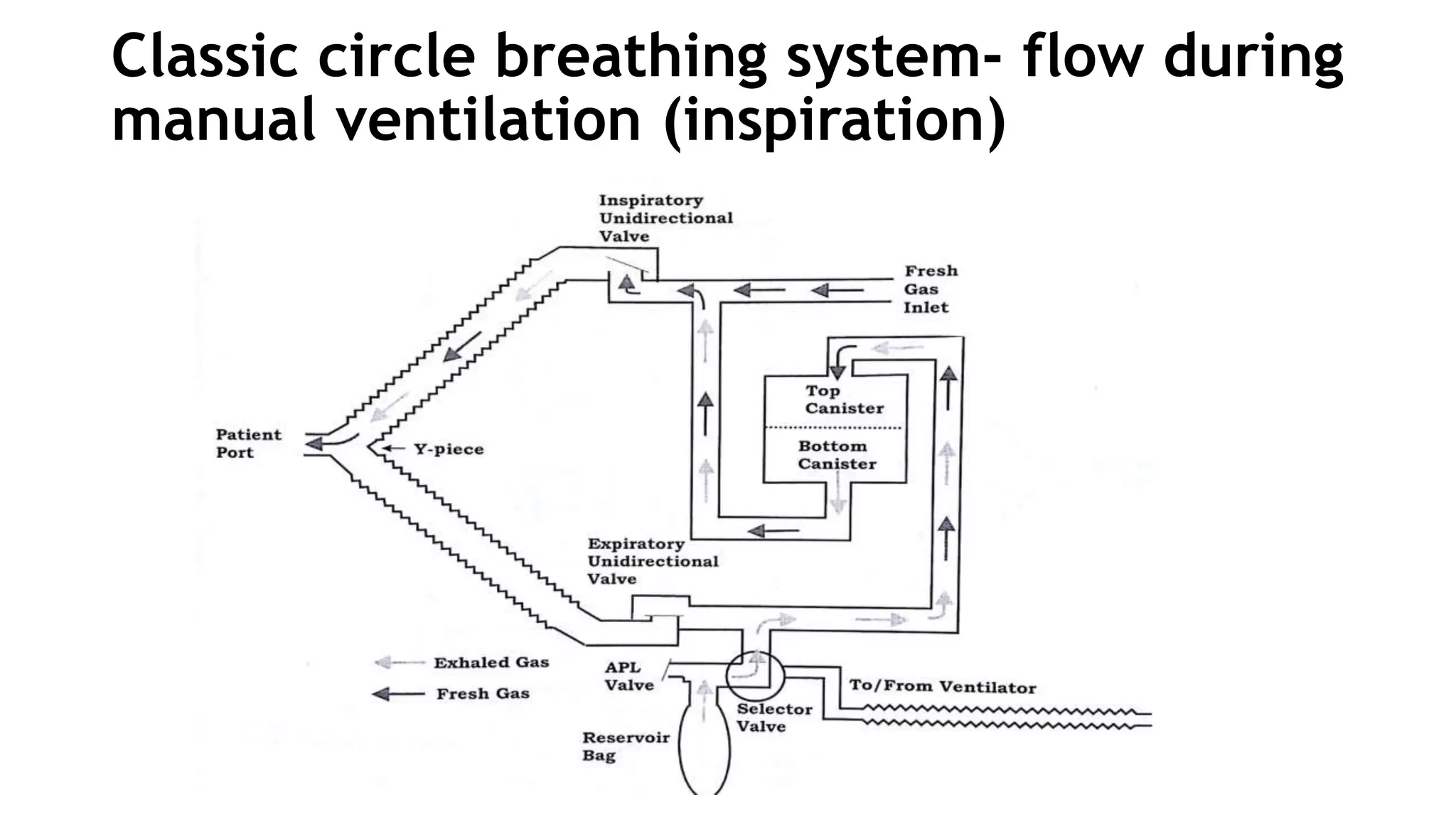
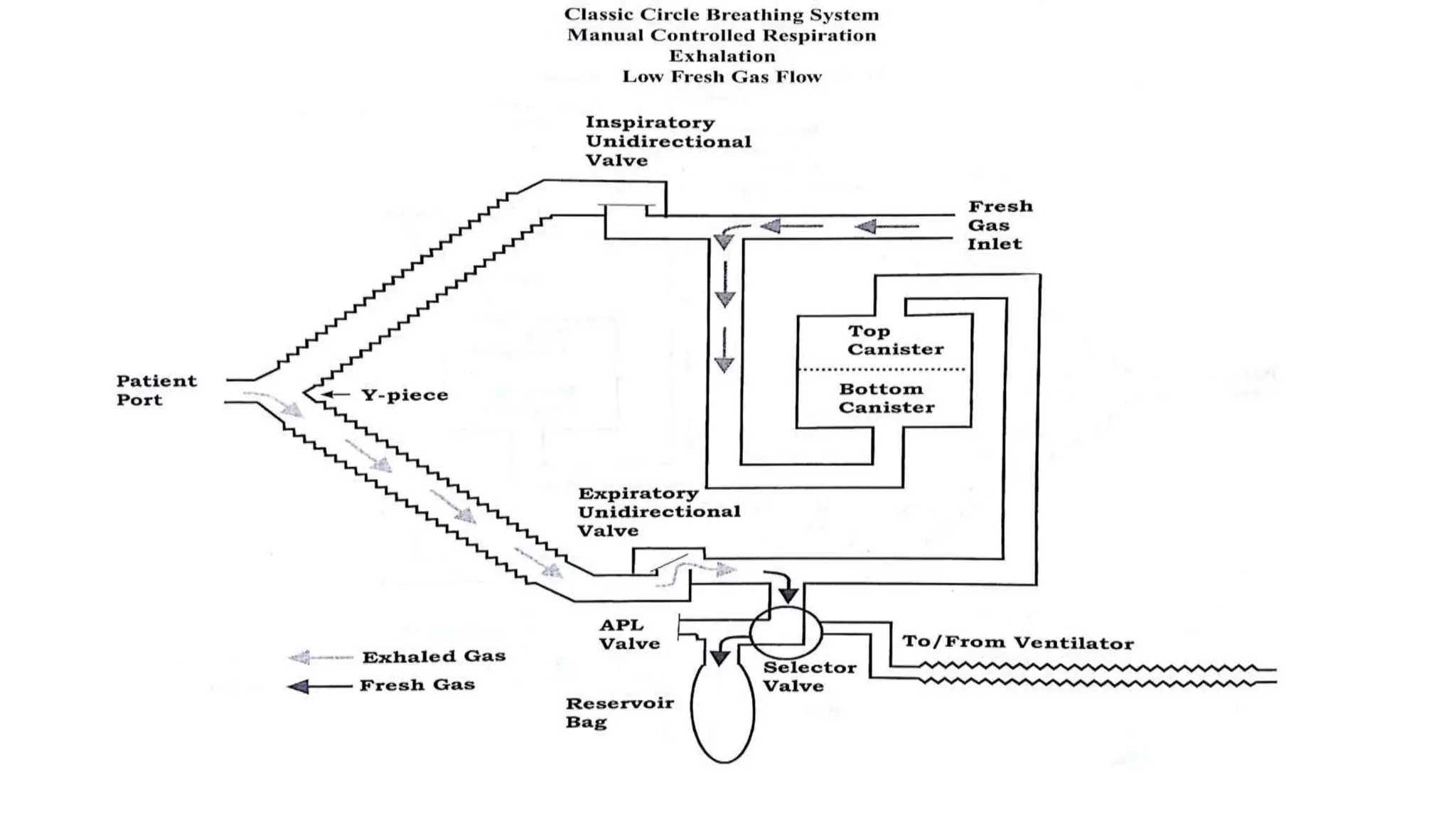
The breathing system delivers gases from the anesthesia machine to the patient's airway. It starts from the fresh gas inlet and ends where gases escape. The circle system uses a circular pathway where exhaled CO2 is removed by an absorbent in the CO2 absorber. Key components include the absorber, unidirectional valves, inspiratory and expiratory ports, fresh gas inlet, Y-piece, APL valve, and breathing tubes. The absorbent, usually sodalime, neutralizes CO2 through an exothermic reaction in the canister. Placement of components and fresh gas flow influences gas flows and absorbent desiccation. The circle system reduces agent use and waste gas exposure while increasing tracheal warmth and



















































































![Maternal Anatomy by _ Dr. tejaswini [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maternalanatomybydr-230122125637-5fc75d39-thumbnail.jpg?width=640&height=640&fit=bounds)



















