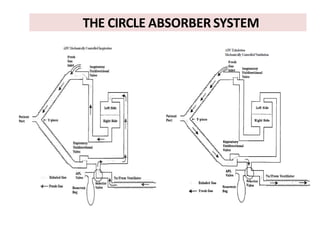
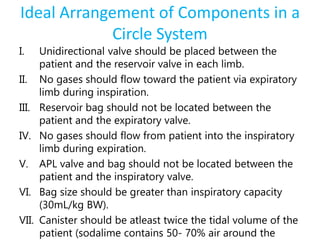
Here are the key components of a circle system:
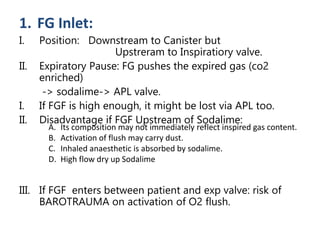
- Fresh gas inlet downstream of the soda lime canister and upstream of the inspiratory valve
- Unidirectional valves
- Breathing tubes
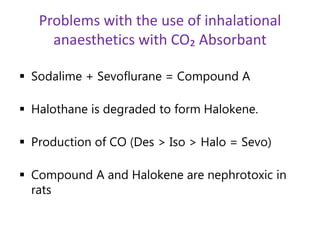
- Soda lime canister for absorbing CO2
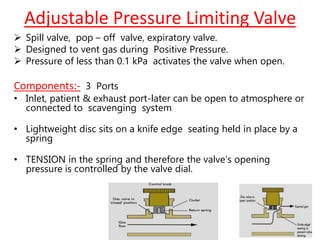
- APL (adjustable pressure limiting) valve
- Reservoir bag or ventilator bellows
- Patient end connection
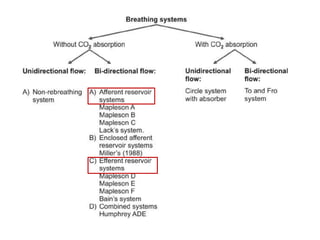
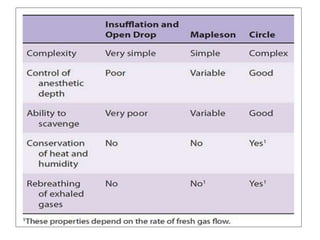
The circle system allows for maximum reuse of gases by ensuring exhaled gases pass through the soda lime canister before being inhaled again. However, it requires higher fresh gas flows to prevent rebreathing. Placement of the fresh gas inlet is important to direct exhaled gases through the soda lime.