Downloaded 30 times




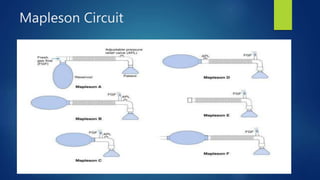
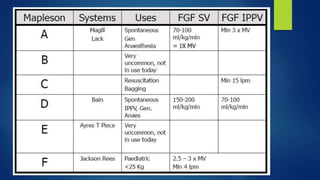



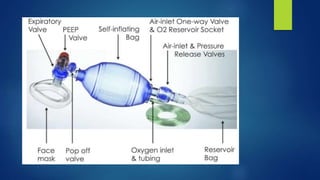

This document describes various components and types of breathing circuits used in anesthesia. It discusses the basic principles of delivering oxygen/gases and eliminating carbon dioxide. The key components described include the reservoir bag, breathing tubes, adjustable pressure limiting valve, and filters. Circuits are classified based on gas flow and include open, semi-open, closed, and semi-closed types. Specific circuits discussed in detail include the Mapleson A-F circuits, Bain's circuit, and the circle breathing system. Advantages and disadvantages of each system are provided.



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















