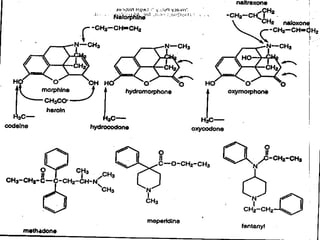
This document summarizes opioids and their classification, mechanisms of action, pharmacokinetics and effects. It discusses both natural and synthetic opioids like morphine, codeine, heroin, fentanyl, hydromorphone, meperidine and methadone. It also covers opioid receptors, endogenous opioid peptides, and antagonists such as naloxone and naltrexone which are used to reverse opioid overdose and effects.



































































![opioids Islamic University [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/opioidsautosaved-250821041508-2c49bca5-thumbnail.jpg?width=640&height=640&fit=bounds)

















![5G Explained! A High Level Overview [Introduction]](https://cdn.slidesharecdn.com/ss_thumbnails/5gexplainedahighleveloverview-260119165306-cc137a3e-thumbnail.jpg?width=640&height=640&fit=bounds)












