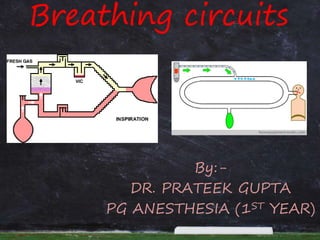
anaesthesia breathing circuits. mapleson circuits. classification of circuits. functional analysia of circuits. draw over circuit. advantages and disadvantages of different circuits.
mapleson circuits used in anesthesia practice, are in their way out but it is as important to know the mechanism with which the gases flow to and fro through them.
mapleson circuits used in anesthesia practice, are in their way out but it is as important to know the mechanism with which the gases flow to and fro through them.
Neuromuscular monitoring, also known as train of four monitoring, is a technique used during recovery from the application of general anesthesia to objectively determine how well a patient's muscles are able to function. It involves the application of electrical stimulation to nerves and recording of muscle response using, for example, an acceleromyograph. Neuromuscular monitoring is typically used when neuromuscular-blocking drugs have been part of the general anesthesia and the doctor wishes to avoid postoperative residual curarization (PORC) in the patient, that is, the residual paralysis of muscles stemming from these drugs.
Neuromuscular monitoring, also known as train of four monitoring, is a technique used during recovery from the application of general anesthesia to objectively determine how well a patient's muscles are able to function. It involves the application of electrical stimulation to nerves and recording of muscle response using, for example, an acceleromyograph. Neuromuscular monitoring is typically used when neuromuscular-blocking drugs have been part of the general anesthesia and the doctor wishes to avoid postoperative residual curarization (PORC) in the patient, that is, the residual paralysis of muscles stemming from these drugs.
A breathing system is a device that conducts gases such as oxygen and anesthetic agents to the patient and conducts waste gases such as CO2 away.
Breathing systems are classified as
Open,
Semi-open,
Semi-closed
Closed.
Semi-closed systems are further divided into
Rebreathing Systems With CO2 Absorption,
Rebreathing Systems Without CO2 Absorption
Non-rebreathing Systems.
More simply, systems can be classified in two groups:
systems with CO2 washout (includes open and semi-open systems)
systems with CO2 absorption (includes closed and semi-closed systems).
lung transplant for covid patients. selection criteria. challenges in covid 19 patients. short term outcomes for patients operated for covid 19 ards. recommendations in covid 19 lung transplant
anaesthesia for lung transplant. indication and contra indication for lung transplant. intra-op and post op complications of lung transplant,
post op pain relief for lung transplant. patient selection for lung transplant. donor criteria for lung donor
central venous pressure and intra-arterial blood pressure monitoring. invasiv...prateek gupta
central venous pressure and intra-arterial blood pressure monitoring. various sites for cvp and Ibp insertion. working principle for cvp and ibp. indication and complication. various waveform of cvp and ibp
Basic principles of MRI machine. effect of mri on monitoring equipments in anesthesia. modes of anesthesia for MRI procedures.safety measures to be taken for MRI procedures
diagnostic criteria and pathophysiology of hellp syndrome. Its anesthetic management both pre-operatively and post operatively. complication and differential diagnosis of hellp
amniotic fluid embolism and cardiac arrest in pregnancyprateek gupta
obstetric emergency. amniotic fluid embolism-pathophysiology,clinical presentation, diagnosis, treatment, laboratory investigations and prognosis. cardiac arrest in preganacy and ACLS 2015 guidelines for CPR and new updates
colloids with their properties and their benefits and disadvantages . indications for colloids. types of colloids and their effect on volume expansio.various studies done for colloids. body fluid compartments and distribution of total body water.
Pulmonary hypertension and its anesthetic managementprateek gupta
pulmonary hypertension and it pathophysiology. pre operative, intraoperative and post operative complications and anesthetic management.
drugs that can be used in anesthetic management of pulmonary hypertensiom
neuromuscular monitoring. different types of stimulation. patterns in both non- depolarizing and depolarizing blocking agents.various tools to assess the degree of block
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
2. WHAT IS IT
• Assembly of components which
connects the patient’s airway to
the anaesthetic machine creating
an artificial atmosphere, from
and into which the patient
breathes.
• A breathing system converts
continuous flow from the
machine to a intermittent flow.
3. INTRODUCTION
• Any resemblance to a
breathing system was
developed by Barth
(1907)
• The Mapleson A (Magill)
system was designed by
Sir Ivan Magill in the
1930's
4. • In 1936, Brian Sword
introduced the circle
system
• Ayre’s T-piece was
introduced in 1937
• Bain Circuit was
introduced in 1972 by
Bain and Spoerel.
5. • Fresh gas entry port, through which
gases are delivered from machine to
system
• Port to connect it to the patient
• Reservoir for gas, to meet peak
inspiratory flow requirements
• Expiratory port through which expired
gas is vented to to atmosphere
• A CO2 absorber
• Corrugated tubes for connecting these
components
7. Criteria ideal system
• ESSENTIAL
1.Delivery of gas from machine to the
alveoli in same concentration as set and in
shortest possible time
2.Effective elimination of CO2
3.Minimal dead space
4.Minimal resistance
8. DESIRABLE
1.Economy of fresh gas
2.Conservation of heat
3. Adequate humidification
4.Efficient during spontaneous
and controlled ventilation
9. CONTD..
5. Efficient for adult, pediatrics and with
mechanical ventilators
6. Light weight
7. Less theater pollution
8. Convenient during use.
10. CLASSIFICATION
• McMOHAN in 1951
• OPEN - no rebreathing
• SEMICLOSED - partial rebreathing
• CLOSED - total rebreathing
11. Dripps, eckenhoff and vandam
• Based on presence or absence of
-Reservoir bag
-Rebreathing
-CO2 absorption
-Directional valve
• Insufflation- gases are delivered directly
into patient’s ariway
12. TYPE INHALATION EXHALATI
ON
RESERVOIR REBREATHI
NG
CO2
ABSORPTN
EXAMPLE
OPEN AIR + AGENT Atmospher
e
- - - Open drop
T-Piece
SEMI-OPEN AIR + AGENT
FROM
MACHINE
Atmospher
e
SMALL MINIMAL
(on FGF)
- T-Piece
with small
reservoir
SEMI-
CLOSED
From
Machine
Atmospher
e+
Machine
large possible + Magill
attachment
Mapleson
systems
CLOSED From
Machine
Atmospher
e+machine
Large Possible + Circle
system
15. BREATHING SYSTEMS
WITHOUT CO2
ABSORPTION
BREATHING SYSTEMS
WITH CO2
ABSORPTION
Bi-directional flow
A) Afferent reservoir
systems.
- Mapleson A,B,C
- Lack’s system.
B) Enclosed afferent
reservoir systems
Miller’s (1988)
Bi-directional flow
To and Fro system.
19. DISADVANTAGE
• FGF has to be constantly adjusted so
uneconomical
• No humidification
• No conservation of heat
• Not convenient because of bulk of valve
• Valve malfunctioning due to
condensation of moisture
20. Bi directional flow
• Extensively used
• Depend on the FGF for effective
elimination of CO2
• FGF
- No FGF - suffocated
- Low FGF - does not eliminate CO2 -
- High FGF - wastage
• FGF should be delivered as near the
patient’s airway as possible.
21. MAPLESON SYSTEM
• 1954 by Professor W W Mapleson
- Maplesons A- (Magills)
- Maplesons B
- Maplesons C
- Maplesons D
- Maplesons E (T-piece)
- Maplesons F (Jackson-Rees
modification of the T-piece)
22.
23. FUNCTIONAL CLASSIFICATION
• Afferent reservoir system (ARS).
• Enclosed afferent reservoir systems (EARS).
• Efferent reservoir systems (ERS).
• Combined systems.
• Enclosed afferent reservoir system has been
described by Miller and Miller.
24. • AFFERENT LIMB - delivers the fresh gas
from the machine to the patient.
• EFFERENT LIMB - expired gas from the
patient and vents it to the atmosphere
through the expiratory valve/port
25. AR SYSTEMS
• SPONTANEOUS BREATHING
- the expiratory valve is separated from
the reservoir bag
- FGF should be atleast one MV
- Apparatus dead space is minimal.
• CONTROLLED VENTILATION
-Not efficient
• FGF close to the expiratory valve
(Mapleson B & C) , the system is
inefficient both during spontaneous and
controlled ventilation
27. MAPLESON A
• Also known as “MAGILLS SYSTEM”
• Best for spontaneous ventilation
• Depend on FGF for CO2 washout so also
known as “FLOW CONTROLLED
BREATHING SYSTEM”
• No rebreathing if FGF=minute volume
• No separation of inspired and expired gases
• Monitoring of ETCO2 is must.
28. • APL valve at patient end.
• FGF and RB at other end of system
• Only one tubing so mixing of gases
• Work of breathing is less
• Length of corrugated tube 110cm /
volume=550ml
29.
30. • FGF requirements
-SPONTANEOUS
• FGF = Minute volume
FGF of 51-85ml/kg/min advised to
prevent re-breathing or 42-88% of
MV
-CONTROLLED
• FGF = 2.5 x MV
31. MAPLESON A
Inspiration
• The valve closes
• Patient inspires FG from the reservoir
bar
• FG flushes the dead space gas towards
patient
32. Expiration
• The pt expires into the reservoir bag
• The initial part of the expired gas is the
dead space followed by alveolar gas
• Meets up with FG, pressure in the circuit
increases forces the APL open
35. • Hence the alveolar gas is rebreathed
before the pressure in the system
increases sufficiently enough to force
the expiratory valve open
• A Fresh gas flow of >20l/min is
required to prevent rebreathing
36. • This system differs from other
circuits in that the fresh gas does
not enter the system near the
patient but near the reservoir bag.
• HAZARD- should not be used with
mechanical ventilator coz entire
system becomes dead space
37. • Test for Mapelson “A”
• Occlude patient end, close APL
valve, pressurize system –
maintaining pressure confirms
integritiy
38. LACK’S MODIFICATION
• In 1976; Lack modified the mapelson
A.
- APL valve at other end
- Added expiratory limb so no
mixing of gas. Two arrangement;
-Dual arrangement (parellel)
-Tube within tube (co-axial)
39.
40.
41. • Tube length 1.5 m
• Outer tube diameter – 30 mm
• Inner tube diameter - 14 mm
• Inspiratory capacity - 500 ml
42. TESTING
• 1)Attach tracheal tube to inner tube at
patient end ; blowing down the tube
with APL valve closed will produce bag
movement if there is leak between two
tubes
• 2) Occlude both limbs at patient end
with APL valve open; squeeze the bag; if
there is leak in inner tube; gas will escape
from APL valve and bag will collapse
43. • Advantages:-
• Location of APL valve- facilitates
IPPV / scavenging.
• Disadvantages:-
• Slight increase in work of breathing.
• Break / disconnection of inner tube-
entire reservoir tube becomes dead
pace.
44. Mapleson B
• Fresh gas inlet near pt and distal to
APL
• APL opens when pressure in the circuit
rises and an admixture of alveolar gas
and FG is discharged
• During Inspiration, a mixture of alveolar
gas and FG is inhaled
• Avoid rebreathing with FGF>2×MV, not
very efficient
45.
46. Mapleson C
• Also known as Water to and fro (Water’s
Circuit)
• Similar in construction to the Mapleson B but
main tubing shorter
• As efficient as Mapleson A if expiratory pause is
minimal
• FGF is equal to 2×MV to prevent rebreathing
• CO2 builds up slowly with this circuit, not
efficient
50. EFFERENT RESERVOIR (ER)
SYSTEMs
• Mapleson’s D, E ,F and bain
circuits
• 6 mm tube as the afferent limb
that supplies the FG from the
machine
• ER systems are modifications of
Ayre’s T-piece
• Work efficiently and economically
for controlled ventilation
51. MAPELSON D
• Incorporates T piece at patient
• RB and APL valve at other end
• FGF enters the system through side arm
of T piece
• FGF required to prevent rebreathing is
1.5-2 times minute volume
• Used for spontaneous and controlled
ventilation
52. BAIN’S SYSTEM
• Described by Bain & Spoerel in 1972
• Modification of Mapelson D system
• Added one more tube; arranged
coaxially
• Inner tube inspiratory;
outer tube expiratory+inspiratory
• Length of tube: 1.8m
• Outer tube diameter: 22mm
• Inner tube diameter :7mm
53.
54.
55.
56.
57.
58. FACTORS THAT TEND TO DEC
REBREATHING (SPONT)
• HIGH I:E RATIO
• SLOW RISE IN INSPIRATORY FLOW
RATE
• A LOW FLOW RATE IN LAST PART OF
EXPIRATION
• A LONG EXPIRATORY PAUSE (BEST)
61. advantage
• Useful for pediatric as will as adult
patient
• Allows warming & humidification of
gases
• useful for spontaneous as will as
controlled ventilation
• Easily dismantled; sterilised; so useful in
infected cases
•
62. Contd.
• Facilitates scavenging
• Length of tubing is long so machine can
be taken away from patient ; useful in
head & neck & Neurosurgery.
• Light weight
• Can be used with ventilator
63. Disadvantage
• High fresh gas flow requirements
• Cannot be used with intermittent
flow machine.
• Disconnection, kink, break, leak, at
inner tube may go unnoticed –
entire exhalation limb becomes dead
space
64. Functional analysis
• During controlled ventilation
-when FGF is high, PaCO2 becomes
ventilatory dependent.
• -when MV exceeds FGF, PaCO2 becomes
dependent on FGF
65. testing
• A) Foex-Crempton Smith test
• Set low flow of O2 on flow meter , close
APL valve
• Occlude the inner tube with a finger or
barrel of syringe at pt end .
• Observe flow meter indicator
• If inner tube is intact and correctly
connected flow meter will fall
• B) Pethik test
• Close APL valve, Activate O2 flush
• Observe the bag
• Due to venturi effect , Bag will deflate .
66. Testing for outer tube
• Close APL valve, occlude the patient
end & pressurize the system. If no
leak pressure will be maintained.
When APL valve is opened the bag
will deflate easily.
67. Ayre's T-piece Designed as a no
valve circuit for paediatrics in
1937 by Philip Ayre. (Later
classified as Mapleson E).
• pic
68.
69. T piece system
• The Mapleson E (T-Piece), has a length
of tubing attached to the T-piece to
form a reservoir
• Uses have decreased because of
difficulties in scavenging
• Still commonly used to administer
oxygen or humidified gas to intubated
patients breathing spontaneously
• There are numerous modifications
70. Mapleson e
• For spontaneous ventilation,the expiratory
limb is left open
• For controlled ventilation,the expiratory
linmb is intermittently occulded and fresh
gas flow inflate the lungs (risk of
barotrauma)
• Rebreathing will depend on the FGF,the
volume of the expiratory limb,the patient’s
minute vent. And the type of ventilation,i.e.
spont versus controlled
71.
72. Mapleson F(Jackson-Rees
System)
• This is a modification of the T-piece with
a bag that has a venting mechanism-
usually a hole
• Adjustable pop-off valve can even be
included to prevent over pressuring
• Scavenging can be done
73.
74.
75. Mapleson F (Jackson Rees)
• For spontaneous ventilation the relief
mechanism is usually left open
• For assisted of controlled ventilation,
the relief mechanism is occluded
sufficient enough to distend the bag,
respiration can then be controlled by
squeezing the bag
76. • The volume of the reservoir bag
should be approximately the
patient’s tidal volume, if the volume
is too large re-breathing may occur
and if too small ambient air may be
entrained
• To prevent rebreathing the system
requires an FGF of 2.5-3 × the
patients Minute volume
78. ADVANTAGES
• Compact
• Cheap
• No valves
• Minimal dead space
• Minimal resistance to breathing/less
work of breathing
• Ventilator can be used
79. disadvantages
• The bag may become twisted and
impede breathing
• High gas flow requirements
80. Relative Efficiency of rebreathing
among various Mapleson circuits
• Spontaneous Ventilation-A>DFE>CB
• Controlled Ventilation-DFE>BC>A
• Mapleson A is most efficient during
spontaneous ventilation, but it is the
worst for controlled ventilation
• Mapleson D is most efficient during
controlled ventilation
81.
82.
83.
84.
85. ADVANTAGES OF MAPLESON
• Simple, inexpensive & rugged
• Variation in MV effect ETCO2 less than
circle
• In Coaxial, Inspiratory limb heated by
warm exhaled gas
• Can be used to ventilate patient in MRI
unit
• Lightweight, no drag on mask or
tracheal tube
86. DISADVANTAGES OF
MAPLESON
• Requires high FGF
• Inspired heat and humidity is low (unless
device is used)
• In A, B, and C APL valve near patient,
hence inaccessible to the operator.
Scavenging is awkward
• Not suitable for malignant
hyperthermia, not possible to increase
FGF enough to remove increased CO2
load
87. insufflation
• The blowing of anesthetic gases across a
patient’s face
• Avoids direct connection between a
breathing circuit and a patient’s airway
• Because children resist the placement of
a face mask or an IV line, insufflation is
valuable
• CO2 accumulation is avoided with
insufflation of oxygen & air at high flow
rate (>10 L/m) under H & N draping at
ophthalmic surgery
• Maintain arterial oxygenation during
brief periods of apnea
88.
89. Draw-over anesthesia
• Non-rebreathing circuits
• Use ambient air as the carrier gas
• Inspired vapor and oxygen
concentrations are predictable &
controllable
• Advantage; simplicity, portability
• Disadvantage; absence of reservoir bag ->
not well appreciating the depth of TV
during spontaneous ventilation
90.
91. Disadvantages of the
insufflation & draw-over
systems
• Poor control of inspired gas
concentration & depth of anesthesia
• Inability to assist or control ventilation
• No conservation of exhaled heat or
• humidity
• Difficult airway management during
• head & neck surgery
• Pollution of the operating room with
large volumes of waste gas
92. COMBINED SYSTEM
HUMPHREY’S ADE system:
• To overcome the difficulties of changing
breathing system for different modes of
ventilation this system is developed
• Two reservoir bag; one in afferent
limb; other in efferent limb; only one is in
use at a time
• System can be changed from ARS
to ERS by changing the position of lever
• Used for adults as will as children
• Functional Analysis same as MAP-A in
ARS& as BAIN in ERS
94. Circle system
• ESSENTIAL CPMPONENT:
• Soda lime canister
• Two unidirectional valve
• FGF entry
• Y piece
• Reservoir bag
• Relief valve
95. CRITERIA FOR EFFICIENT
FUNCTIONING
• Two unidirectional valve on either side
of RB
• Relief valve on expiratory limb
• FGF should enter proximal to
inspiratory unidirectional valve
96.
97.
98. TESTING
• Set all the gas flows to zero.
• Close APL valve
• Occlude Y piece
• Pressurize system to 30cm of with
Oxygen flush
• Pressure should remain fixed for at least
10 sec.
• Open APL valve and ensure pressure
decrease
99. ADVANTAGES
• Exhaled gas–CO2 used again and again
• Constant inspired concentration
• Conservation of heat & humidity
• Useful for all ages
• Useful for low flow ;reduces cost of
Anaesthesia
• Low resistance
• Less OT pollution
•
100. DISADVANTAGES
• Increased dead space
• Malfunctioning of unidirectional valve
• Exhausted soda lime; danger of
hypercarbia