Downloaded 693 times

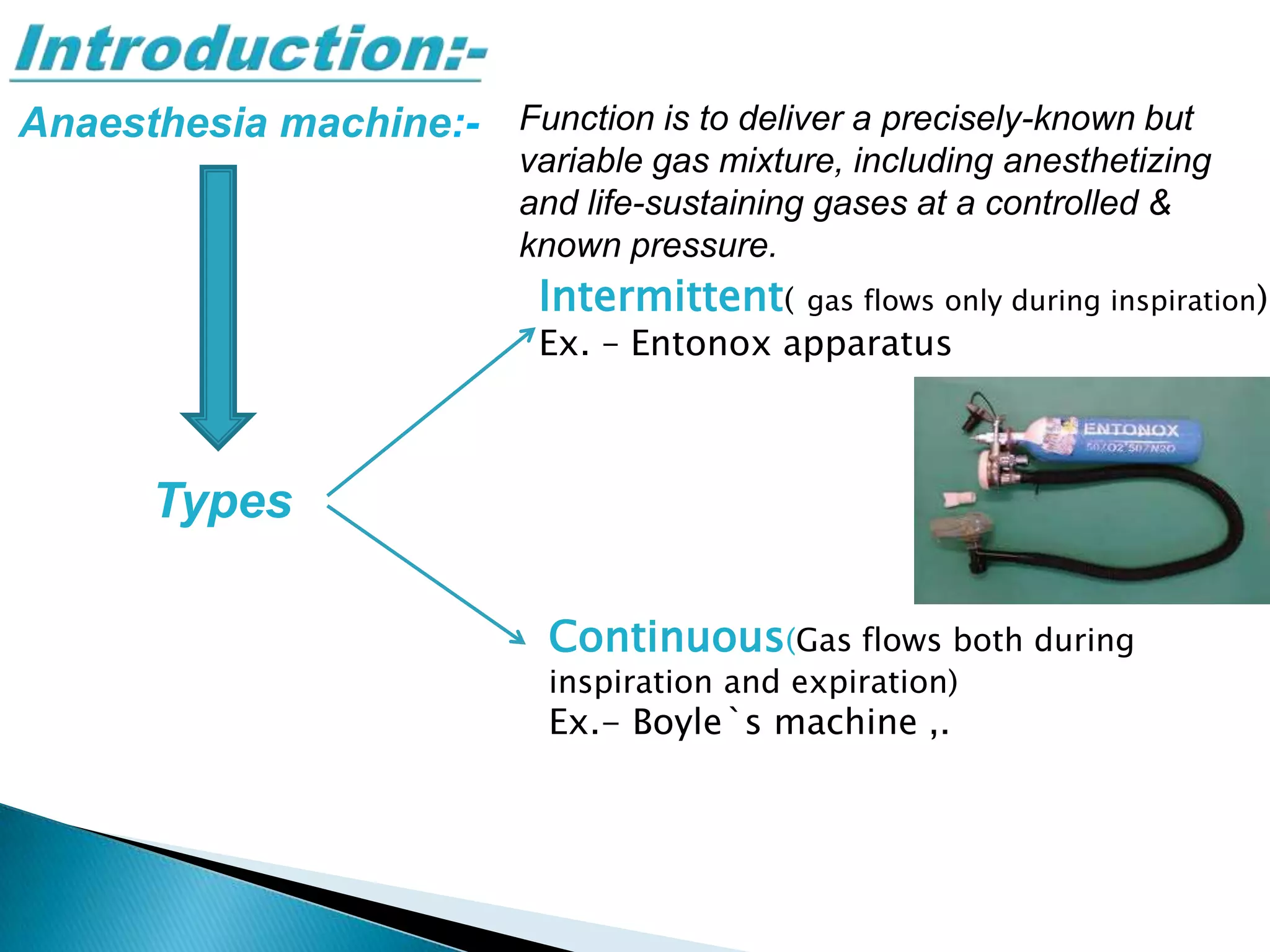
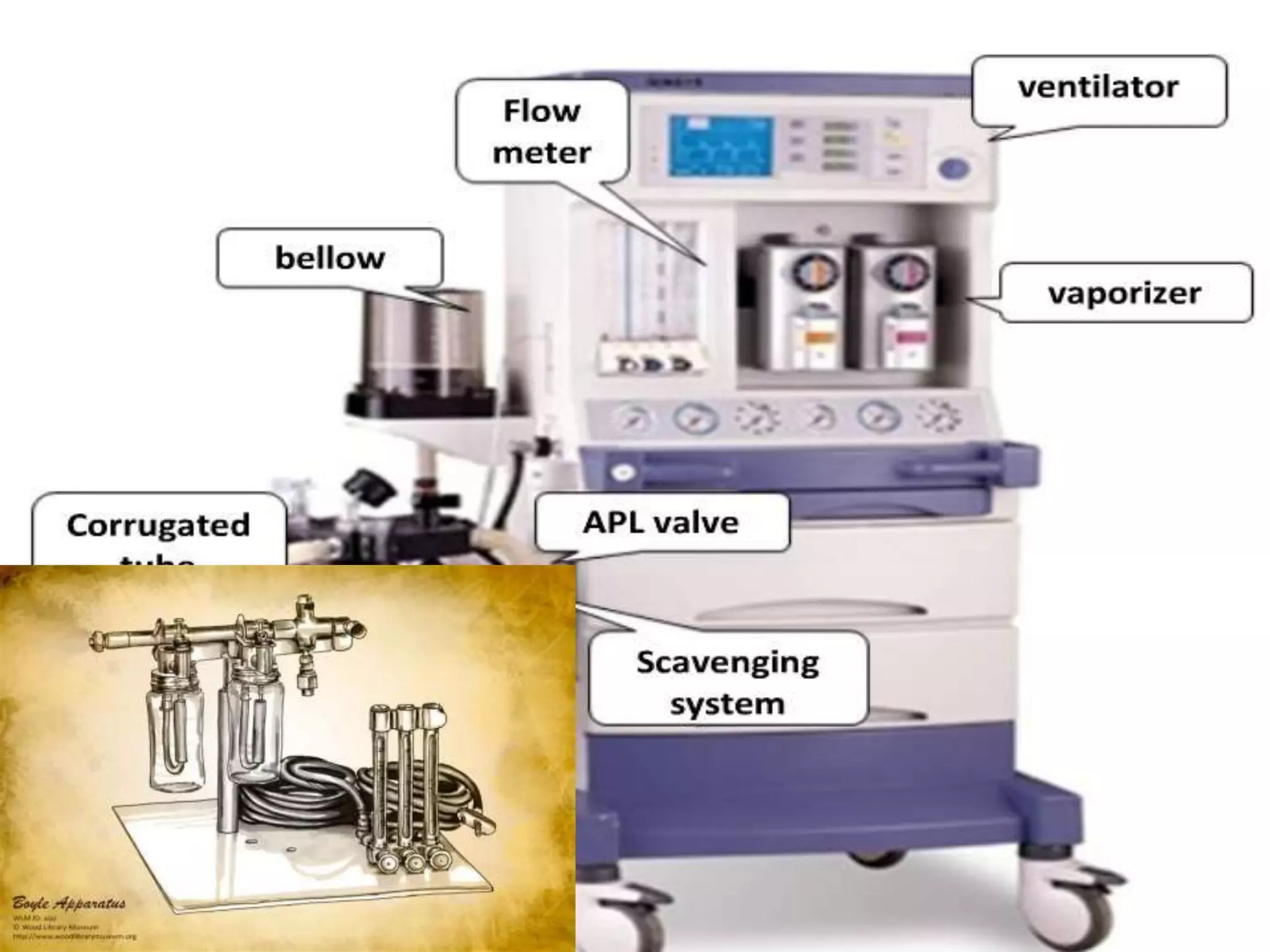
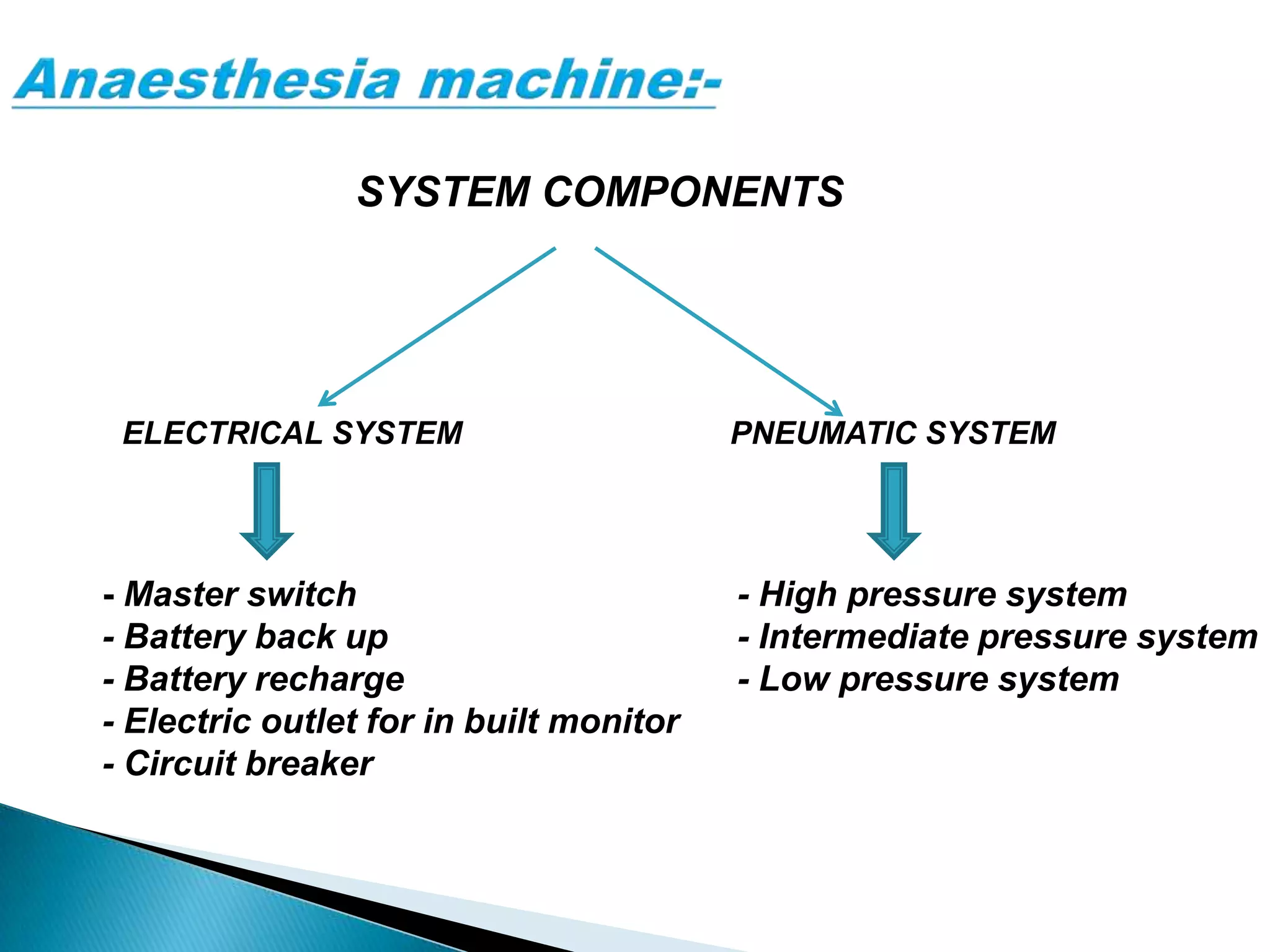
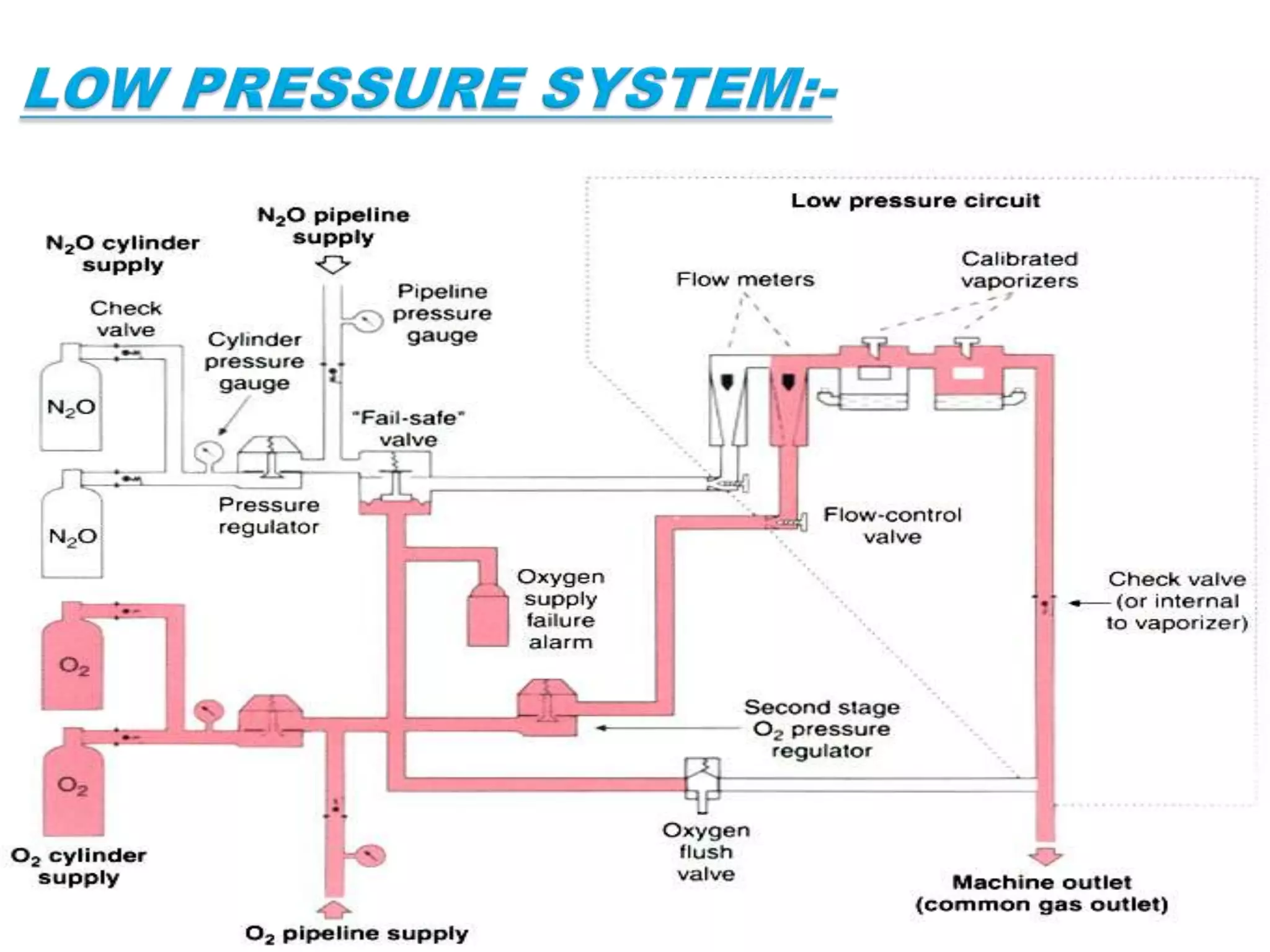

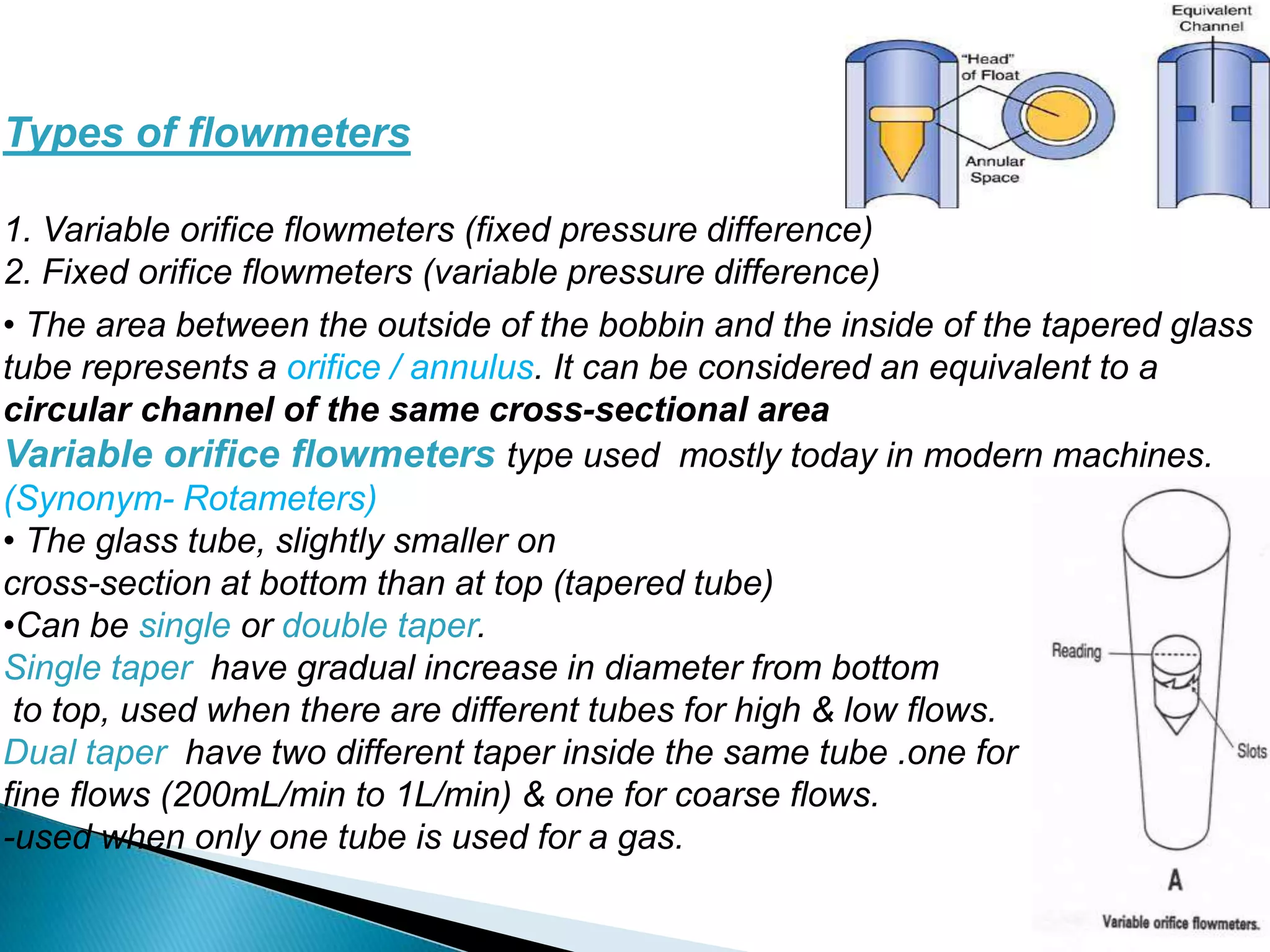
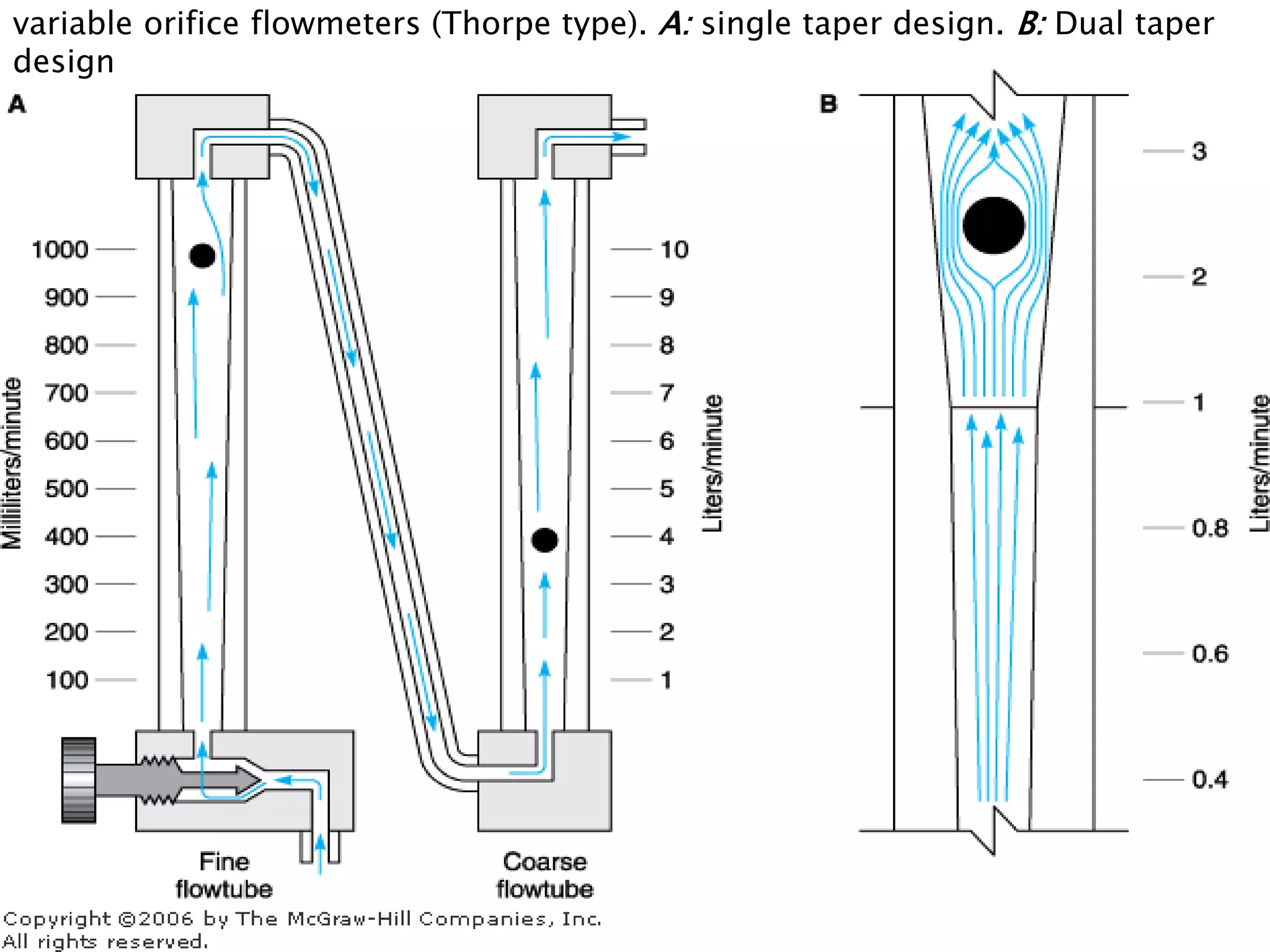

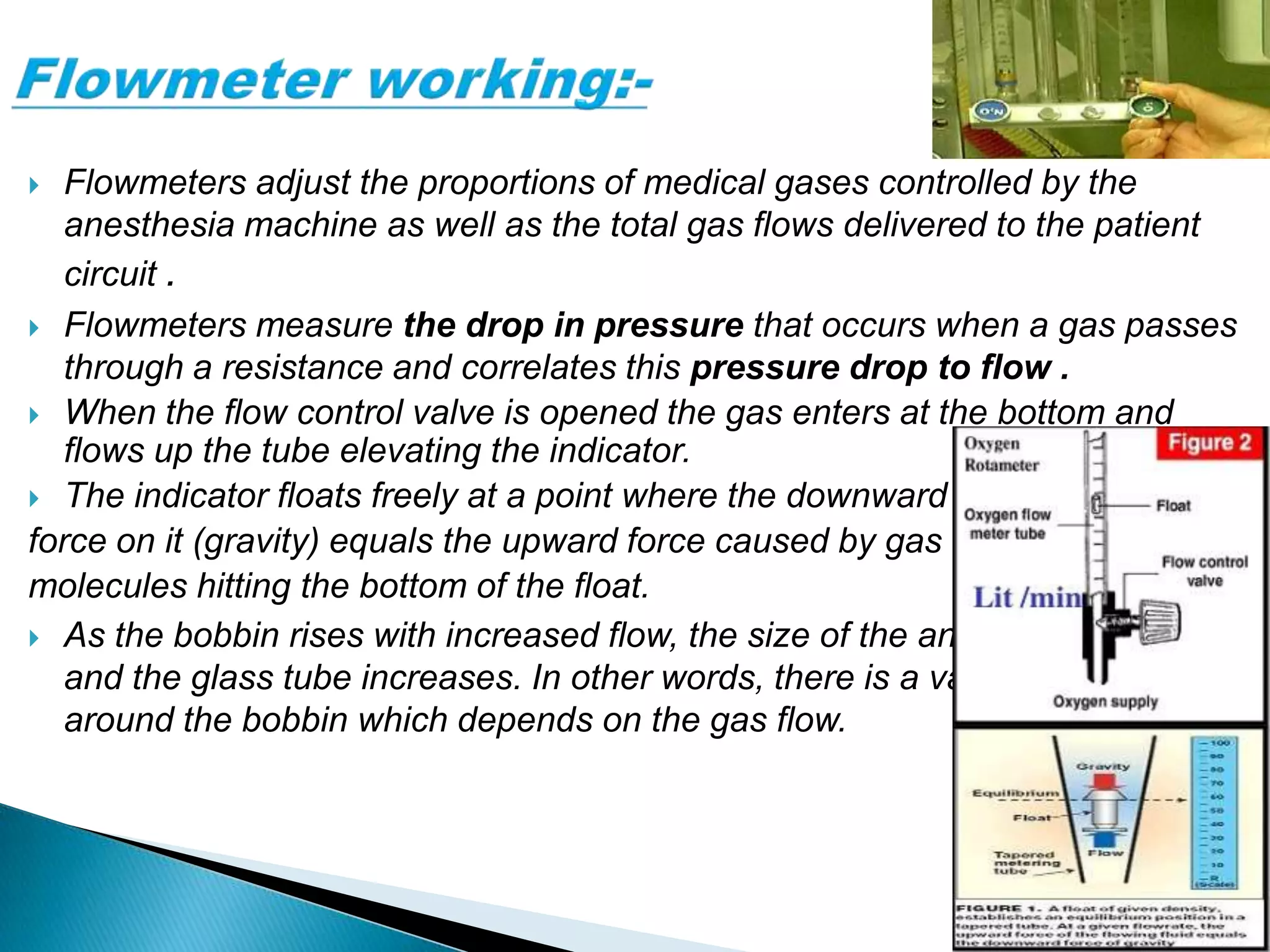



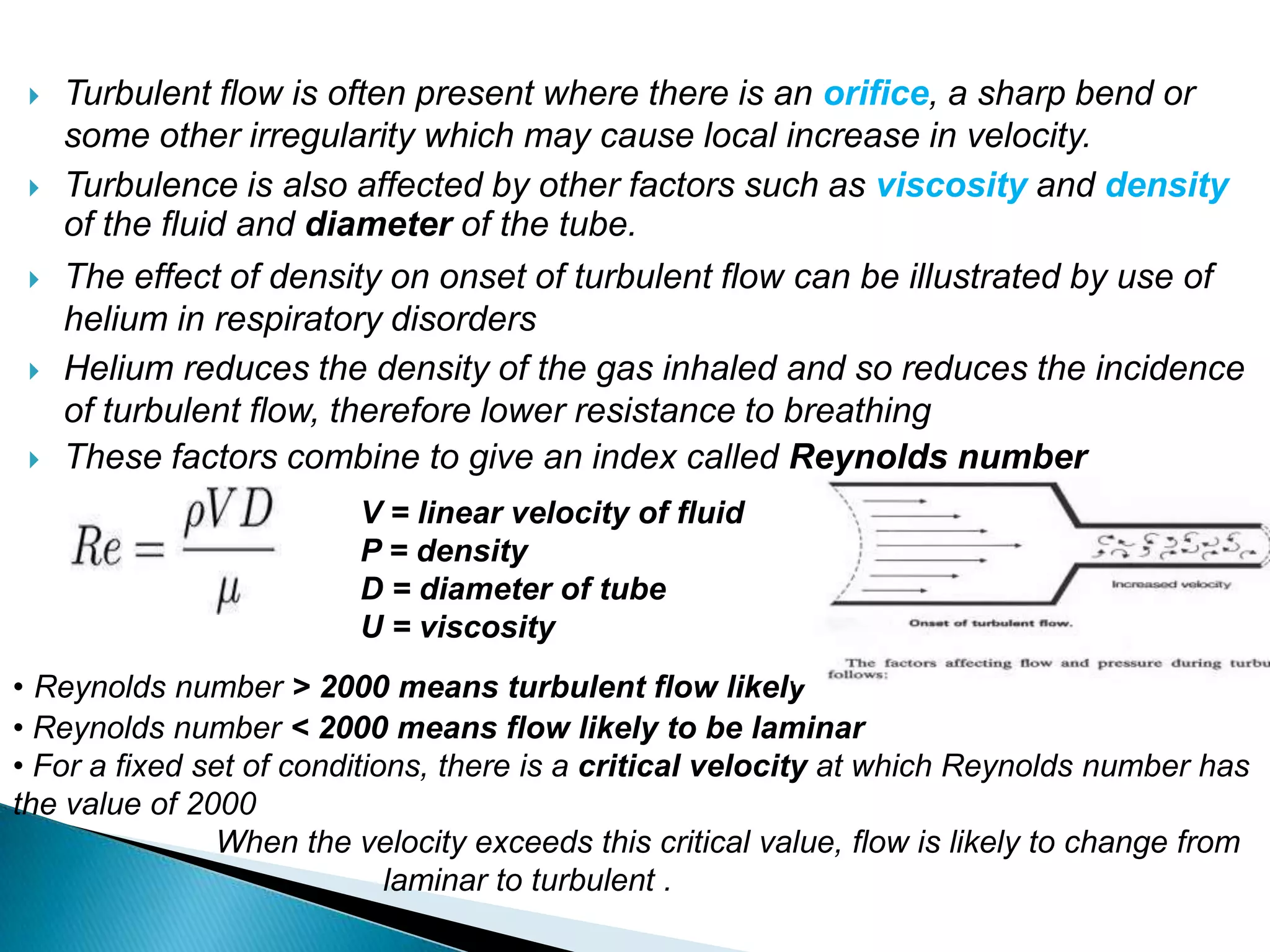
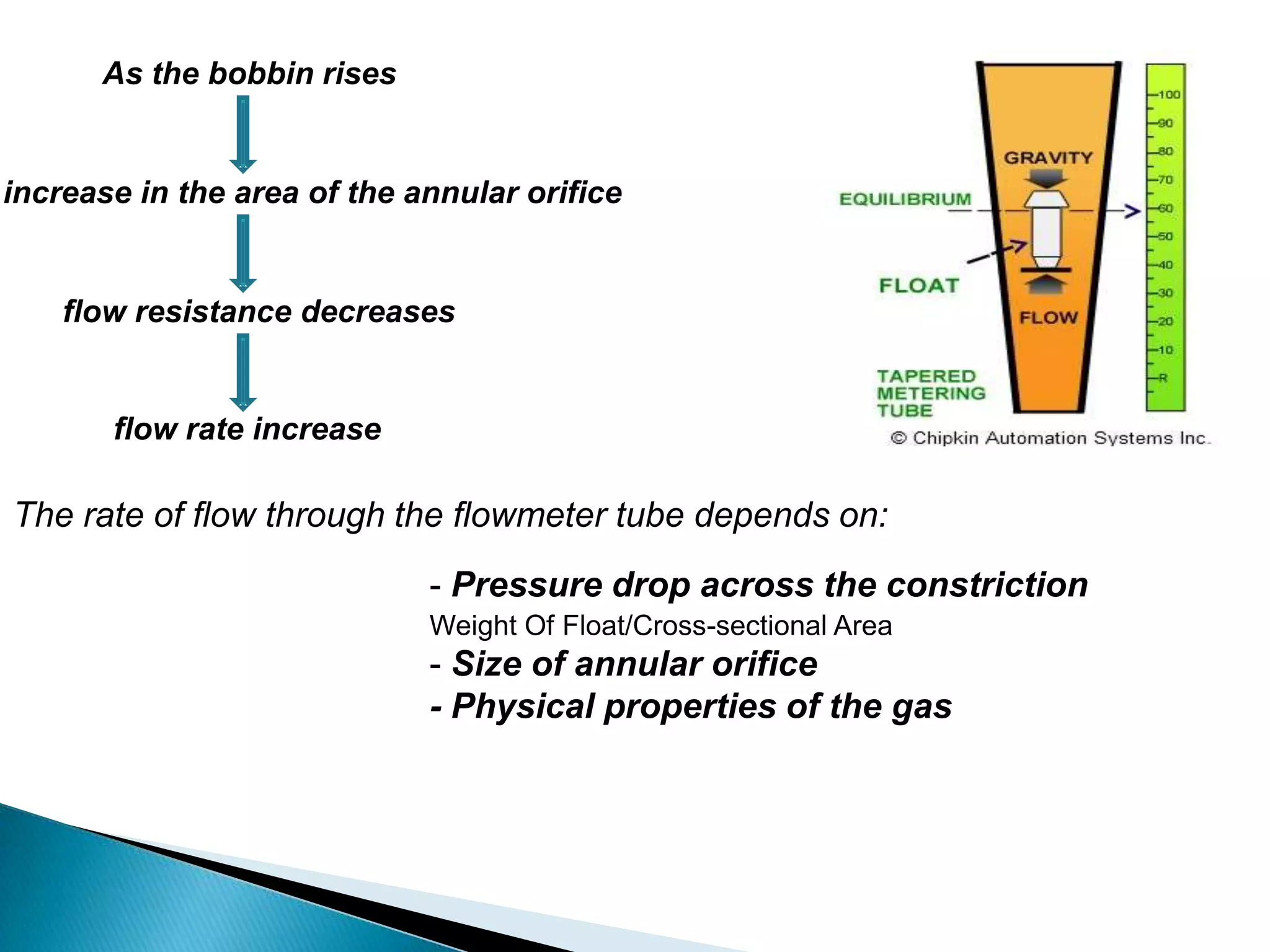
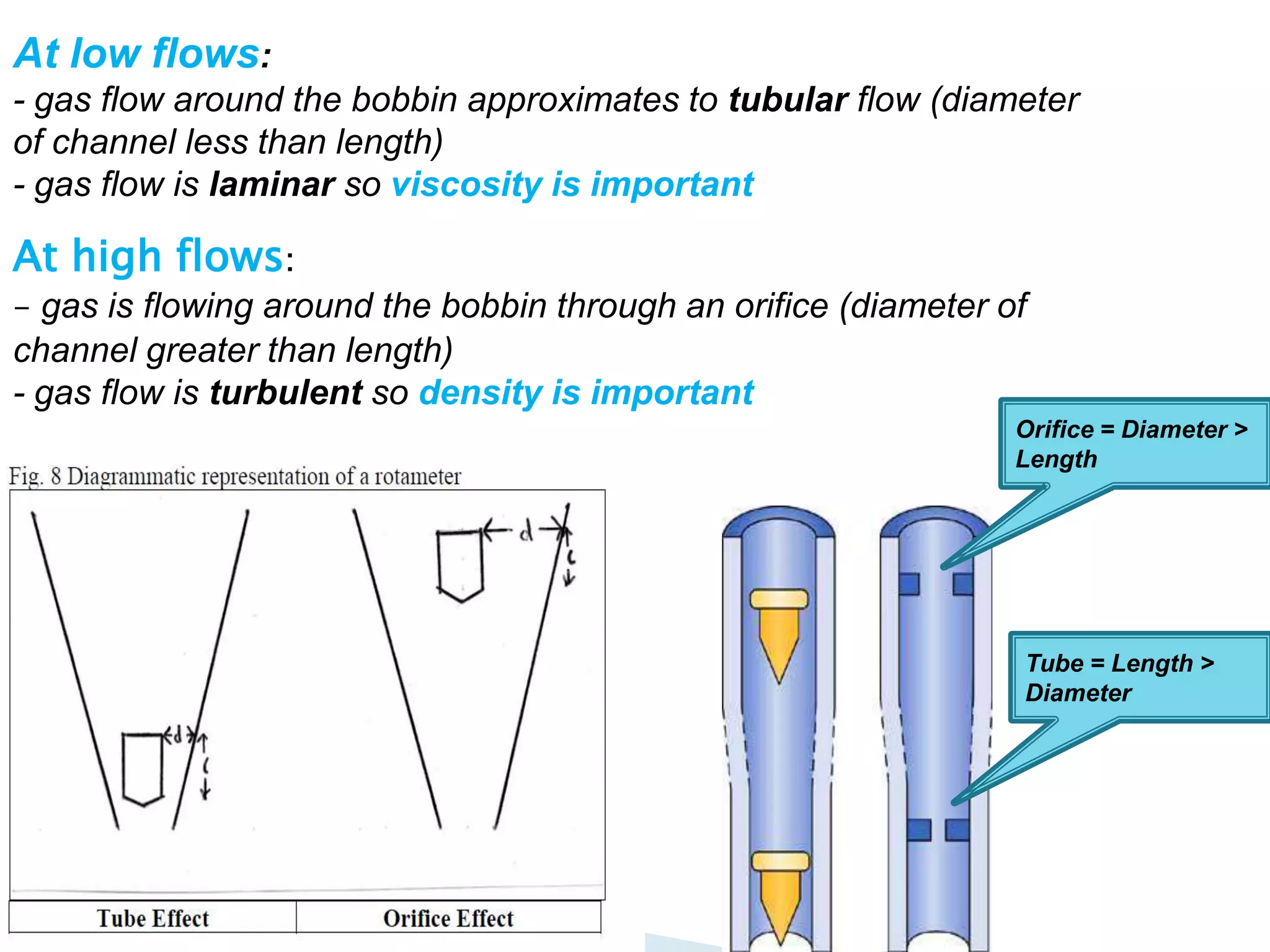

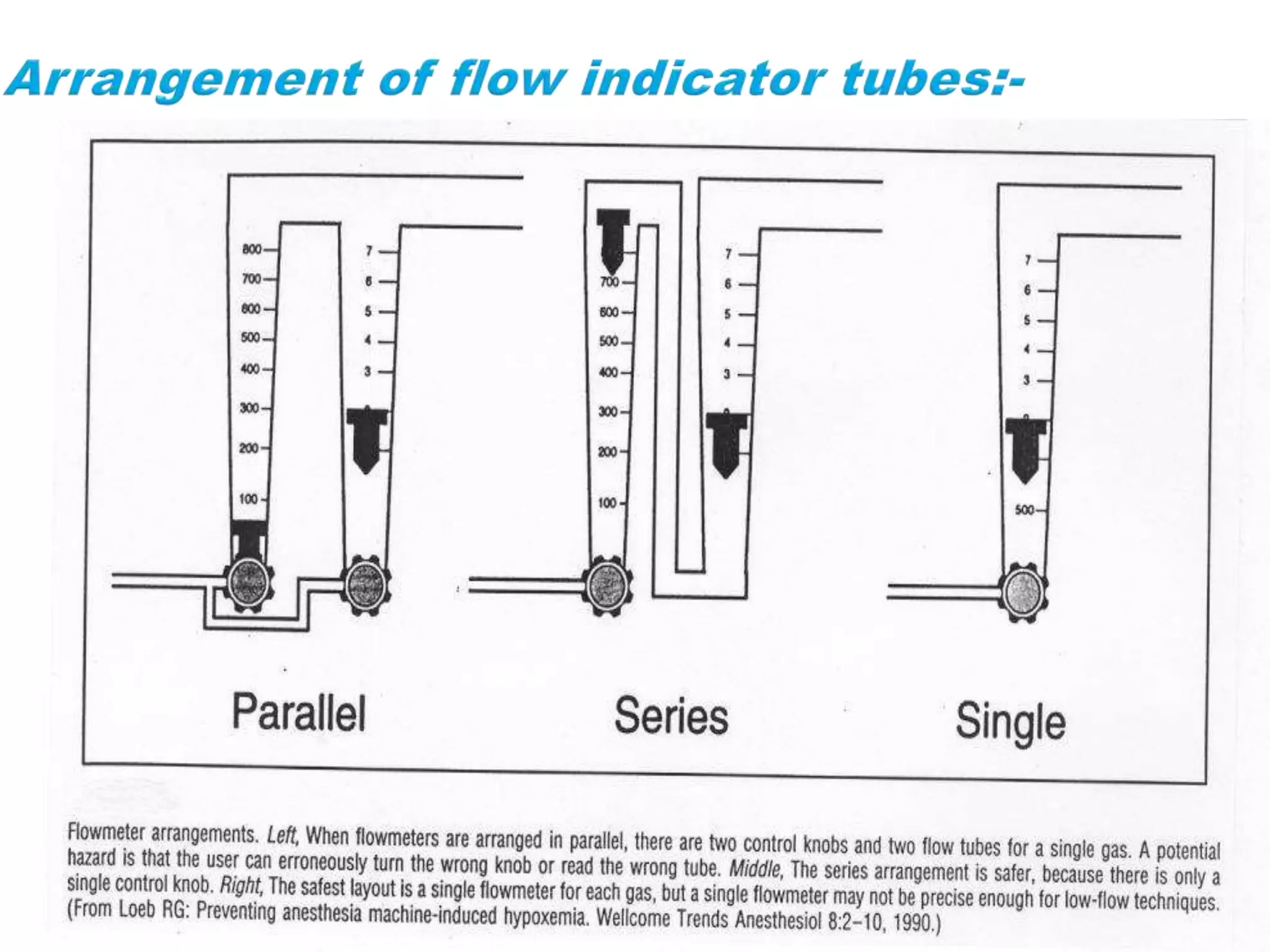
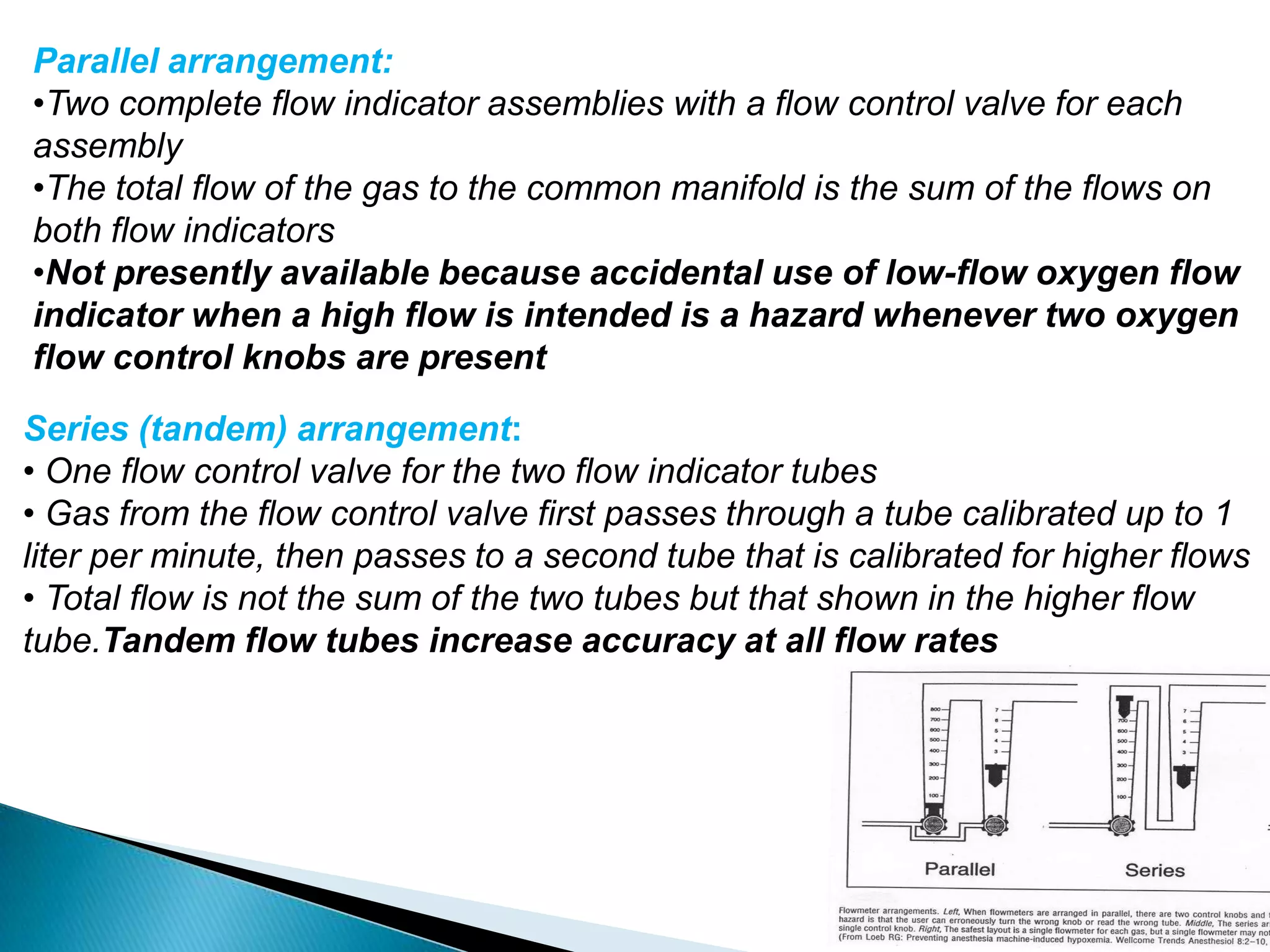



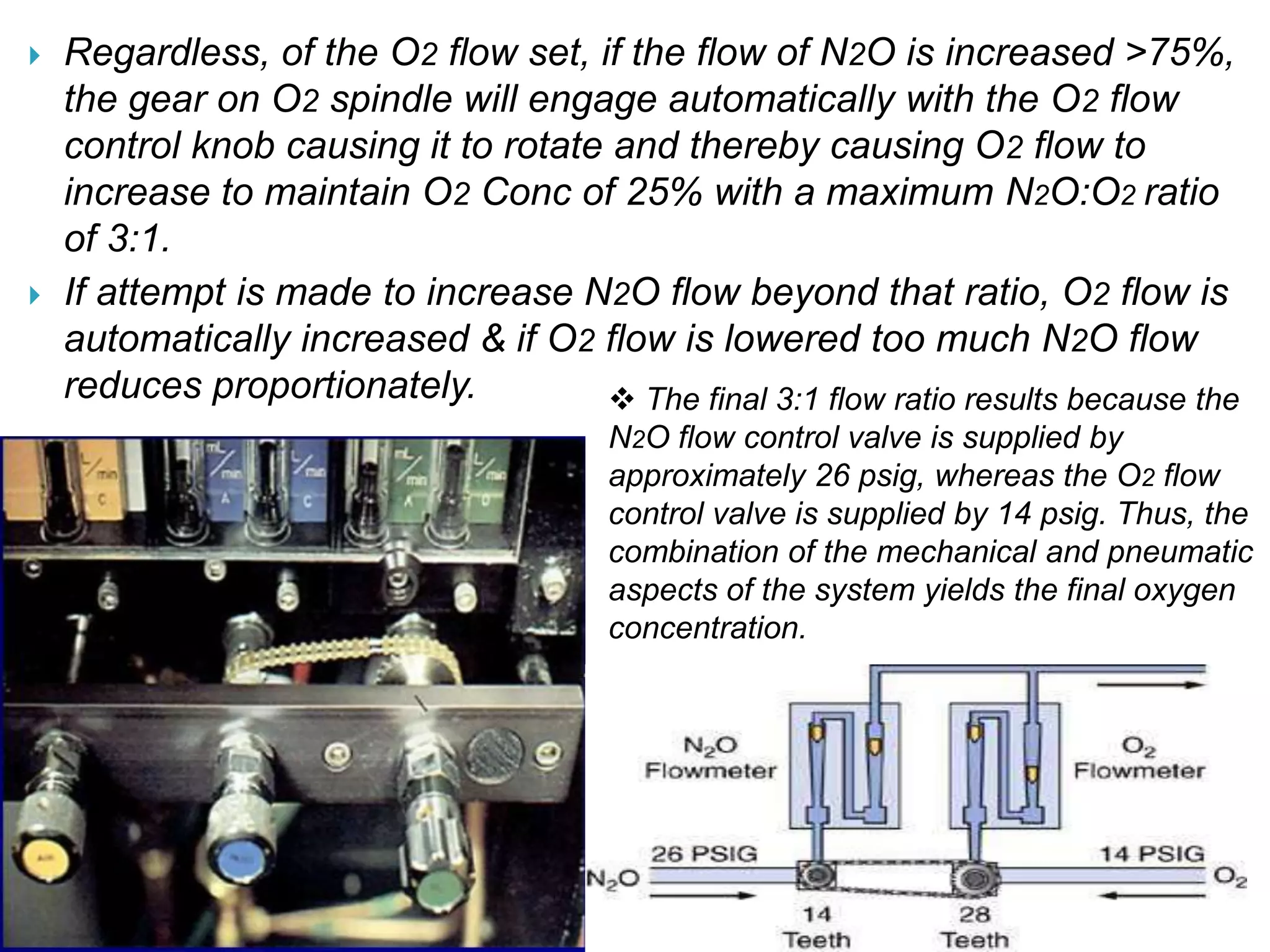



This document provides information about Boyle's anesthesia machine. It discusses the components and functions of an anesthesia machine, including the pneumatic and electrical systems. It describes the different parts of the machine like the flowmeters, vaporizers, check valves, and safety features. The document explains how flowmeters work using the Hagen-Poiseuille equation and factors like viscosity, density, and laminar vs turbulent flow. It discusses temperature and pressure effects on flowmeters as well as protections against delivering a hypoxic gas mixture to the patient.
















































































