Downloaded 387 times

![Low Vision
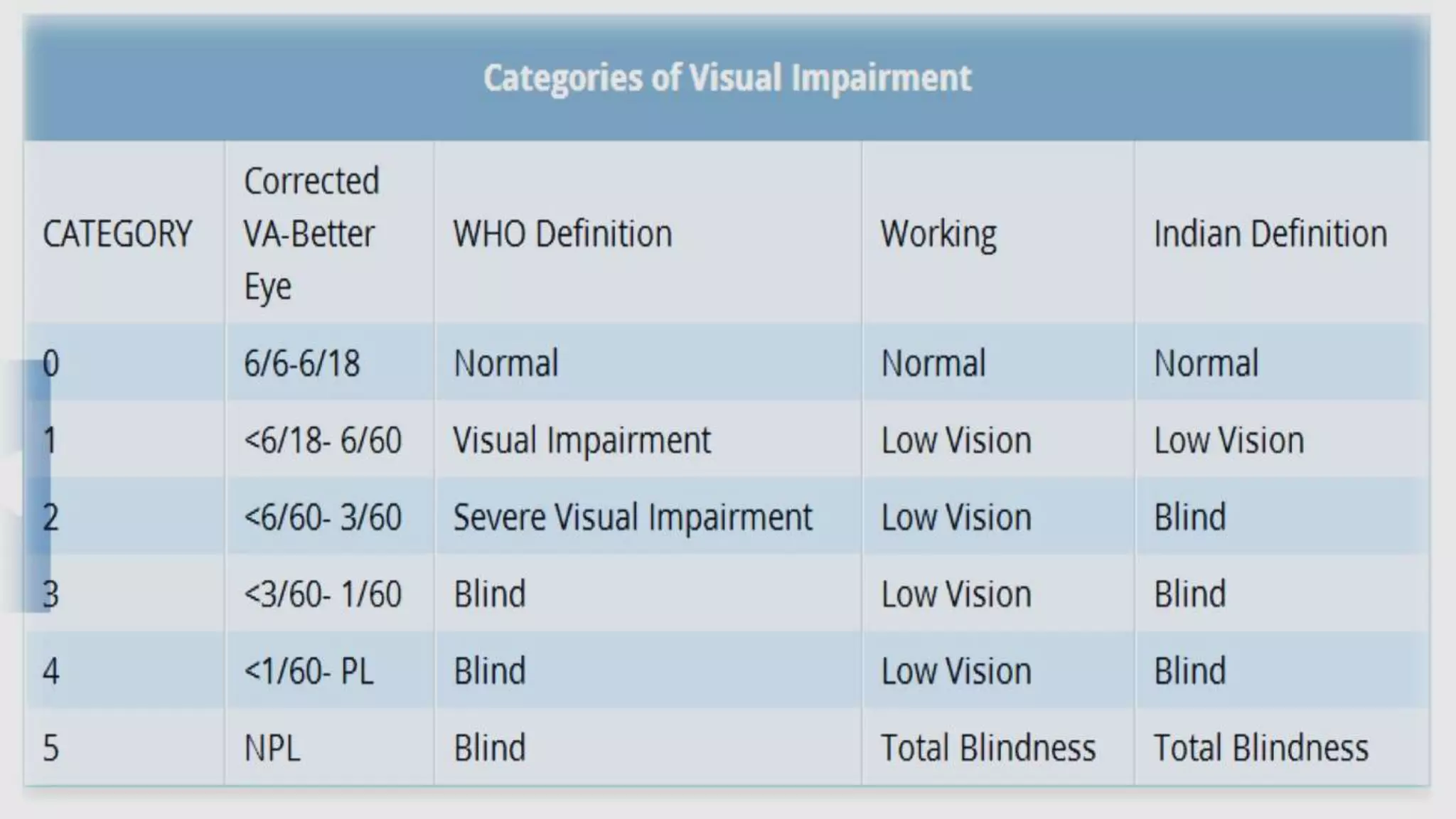
• Low vision essential refers to :
• “Level of vision that prevents a person from performing customary
vision activities with standard or conventional optical correction”
• ICD : Visual Impairment – [Maximum Visual Loss less than
6/18 snellen in better eye/ field of vision of 10 degree or less]
divided into 5 categories](https://image.slidesharecdn.com/lowvisuaaids-140810044650-phpapp01/75/Low-visual-aids-2-2048.jpg)





















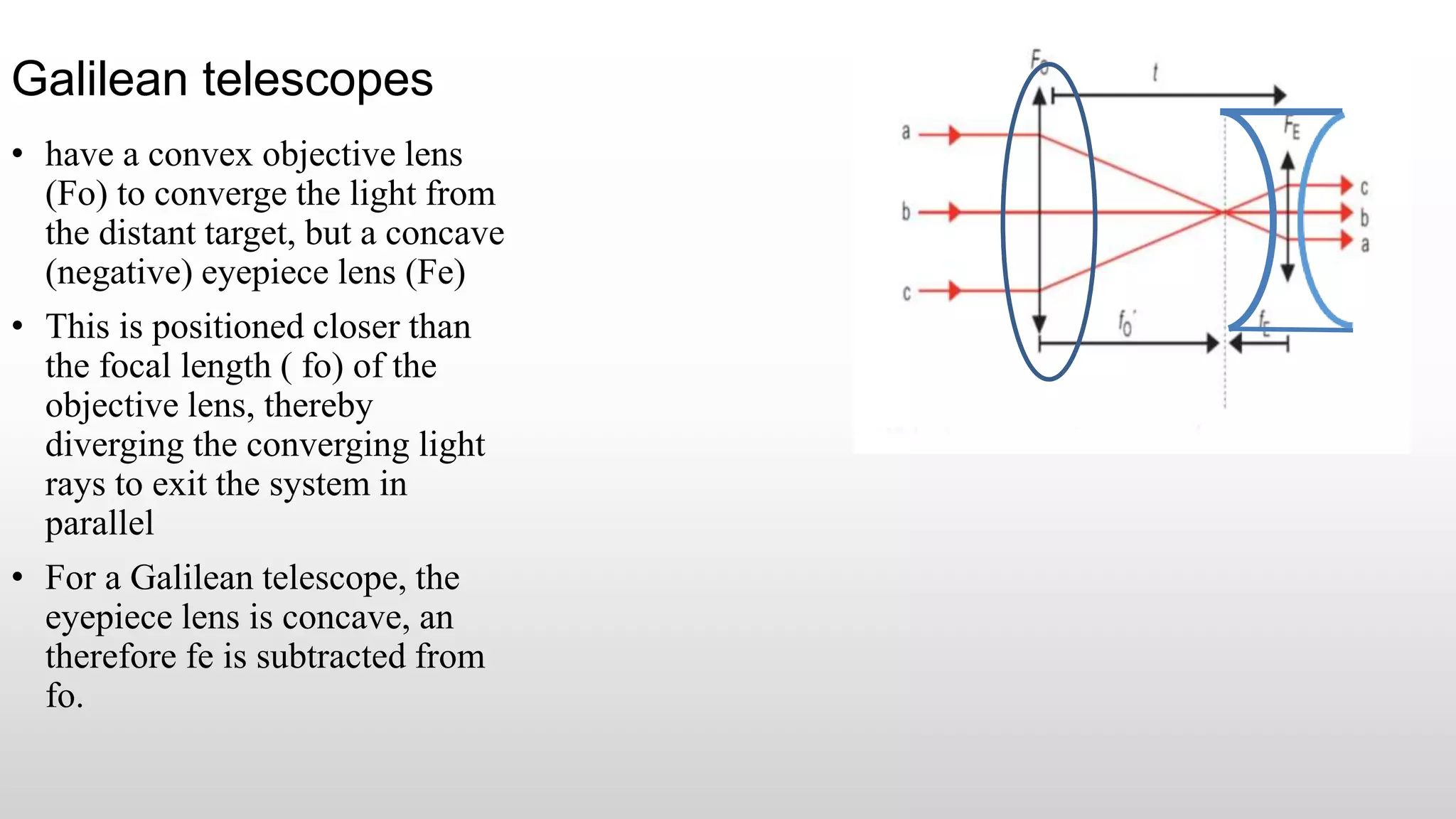
![Astronomical telescopes
[Keplerian] telescopes
• Consist of two convex (positive) lenses;
the first (Fo) converges the light so that
the rays reverse when they pass the
lenses focal length ( fo)
• Second eyepiece lens (Fe) converges the
now divergent rays so that they are
parallel when exiting the system
• The image is inverted, a situation that is
rectified, both laterally and vertically, by
prisms
• For an astronomical telescope, both
lenses are convex and therefore both fo
and fe are positive](https://image.slidesharecdn.com/lowvisuaaids-140810044650-phpapp01/75/Low-visual-aids-33-2048.jpg)













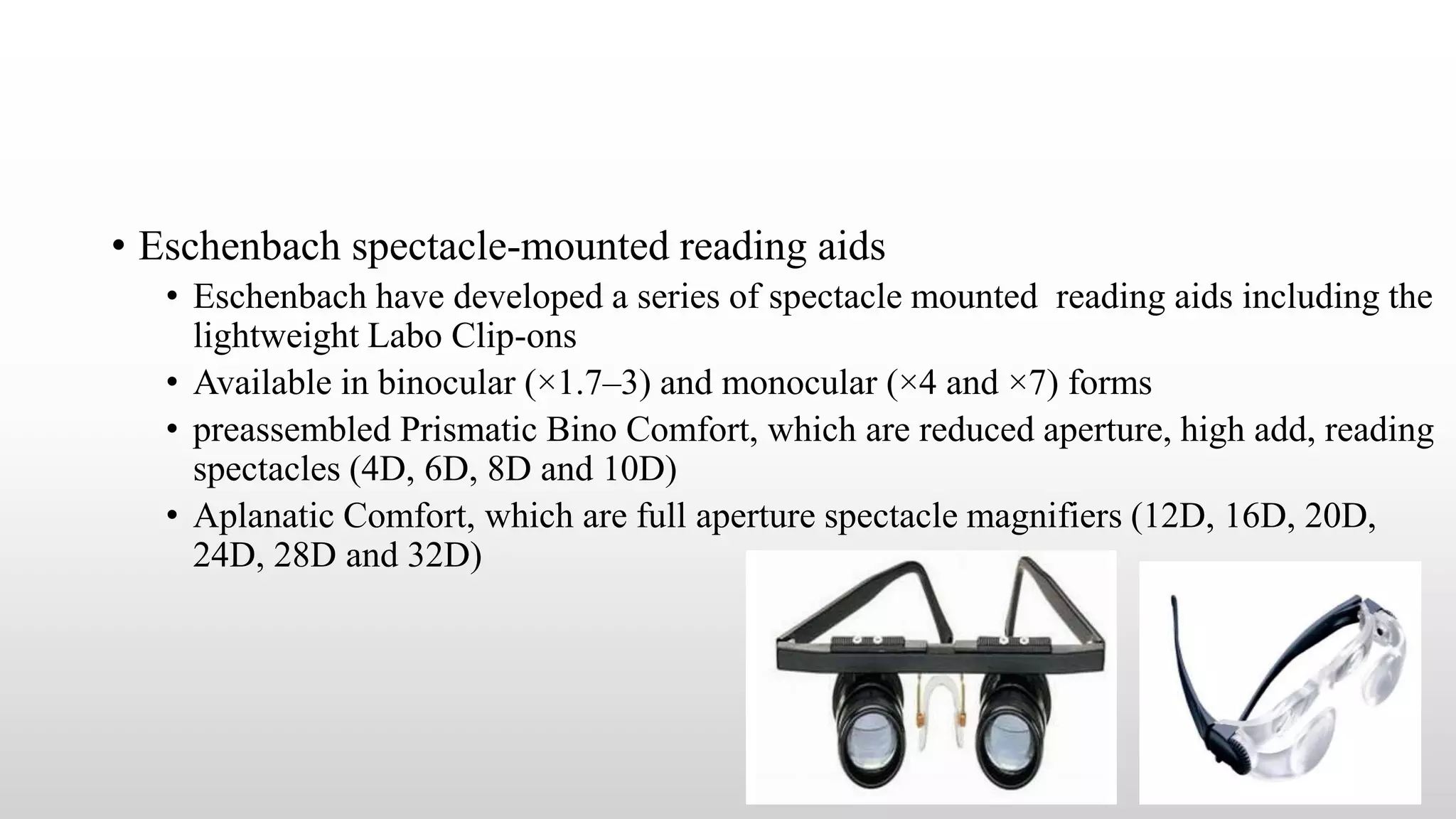
![Dispensing LVA
• Magnifiation trial
• Magnification required should be calculated taking into influence of scotometry, contrast and glare
data
• Power of reading correction should be adjusted until the patient can read the target size words and text
• Presciption of Appropiate devices
• Various LVAs of the calculated power should be testes systematically in sequence : Convex lens first as
a spectacle [either monocular/ binocular with converging prisms]
• Second as a hand magnifier and third as a stand magnifier
• Complex telescopes, microscopic doublet, electronic systems should be reserved as last choice
• Final Choice depends on Patients compability
Training to use appropriate LVA
• Patient should be taught how to handle the aid, how to hold the printed material,
Working distance
• Should be educated regarding optimal Lightning , take care of the device
• Counselling and motivation of the patient for the continue use of LVA
• Periodic Follow up – User performance with the aid, amount of progression made](https://image.slidesharecdn.com/lowvisuaaids-140810044650-phpapp01/75/Low-visual-aids-53-2048.jpg)



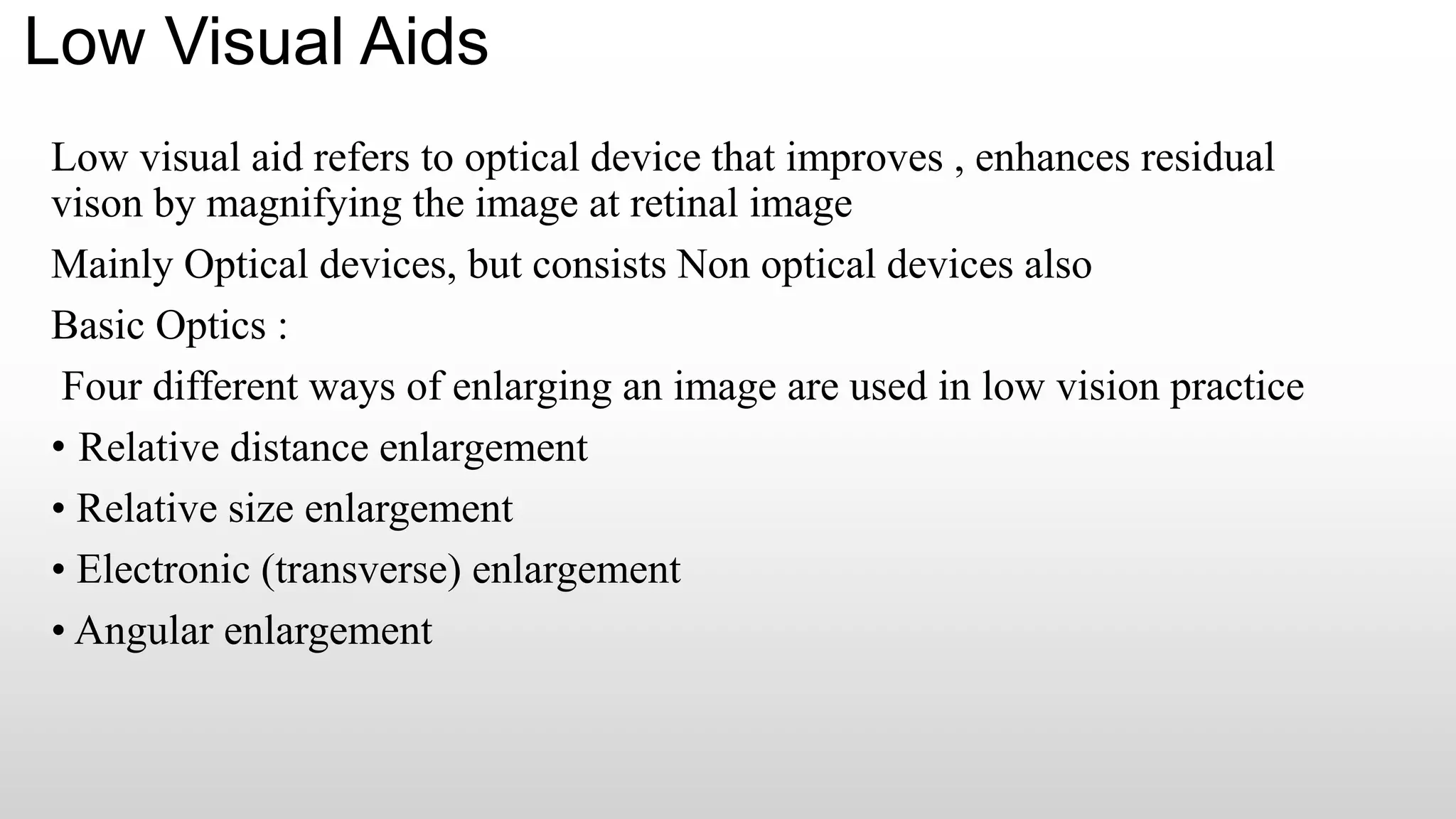
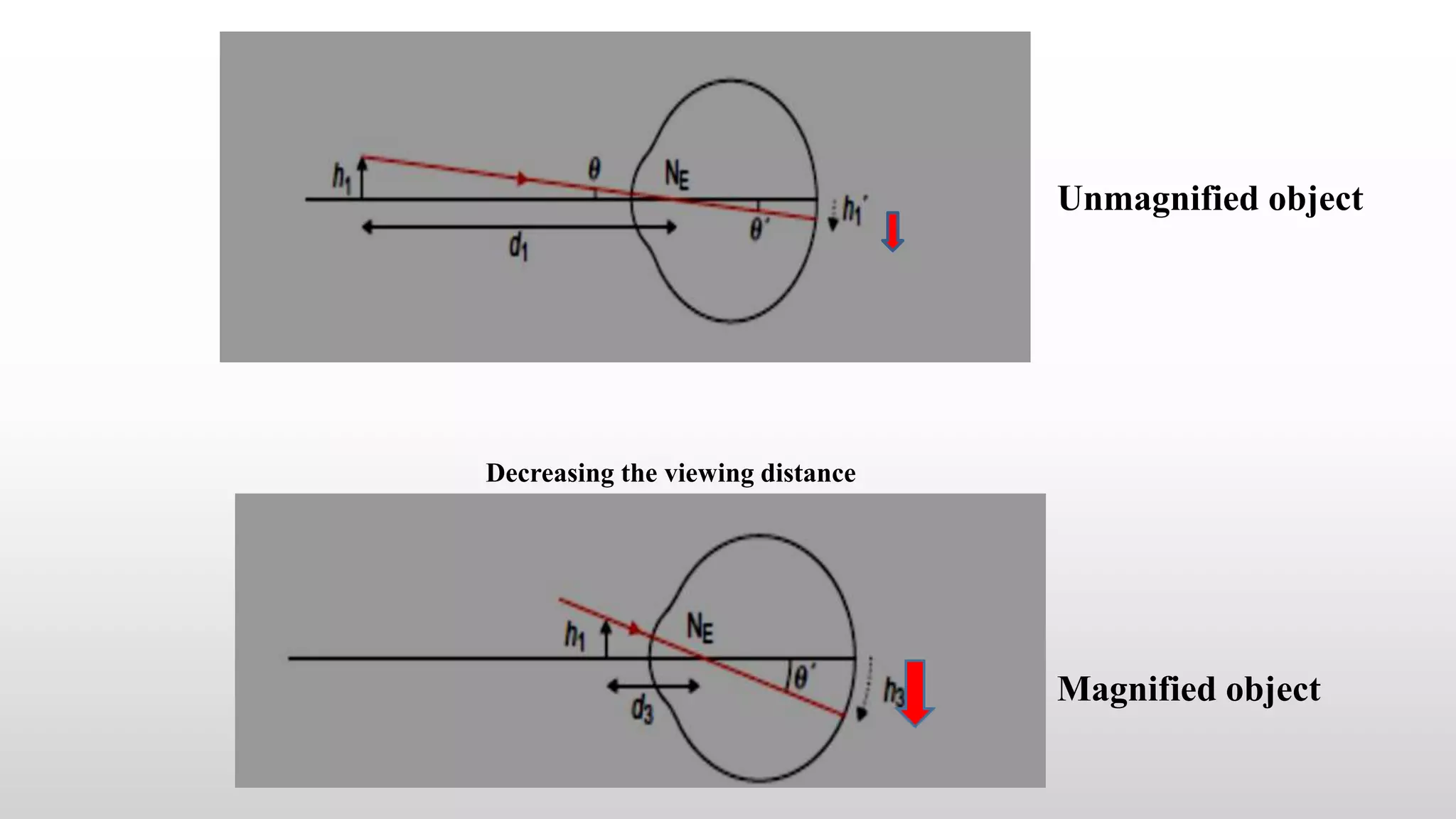
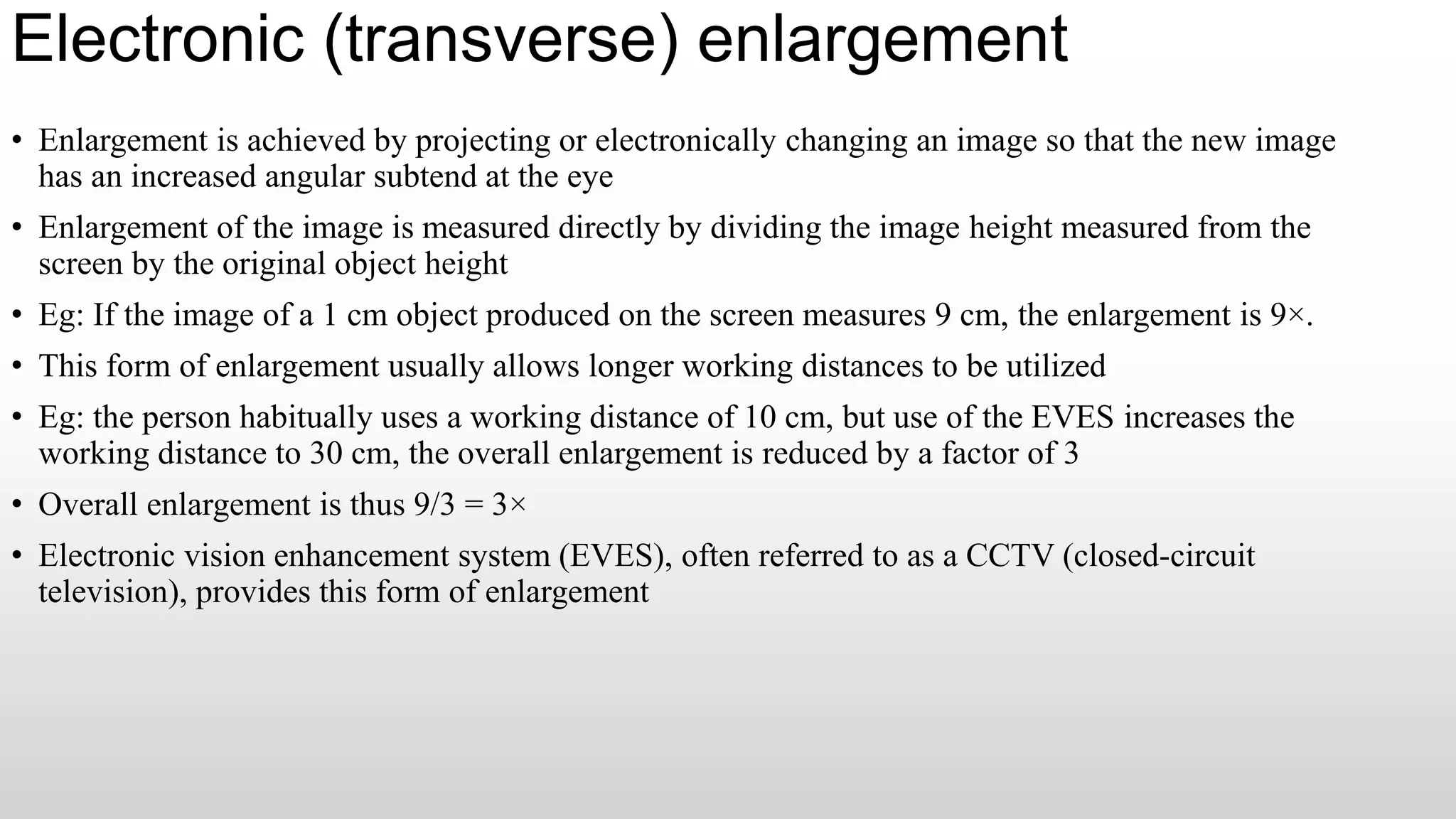
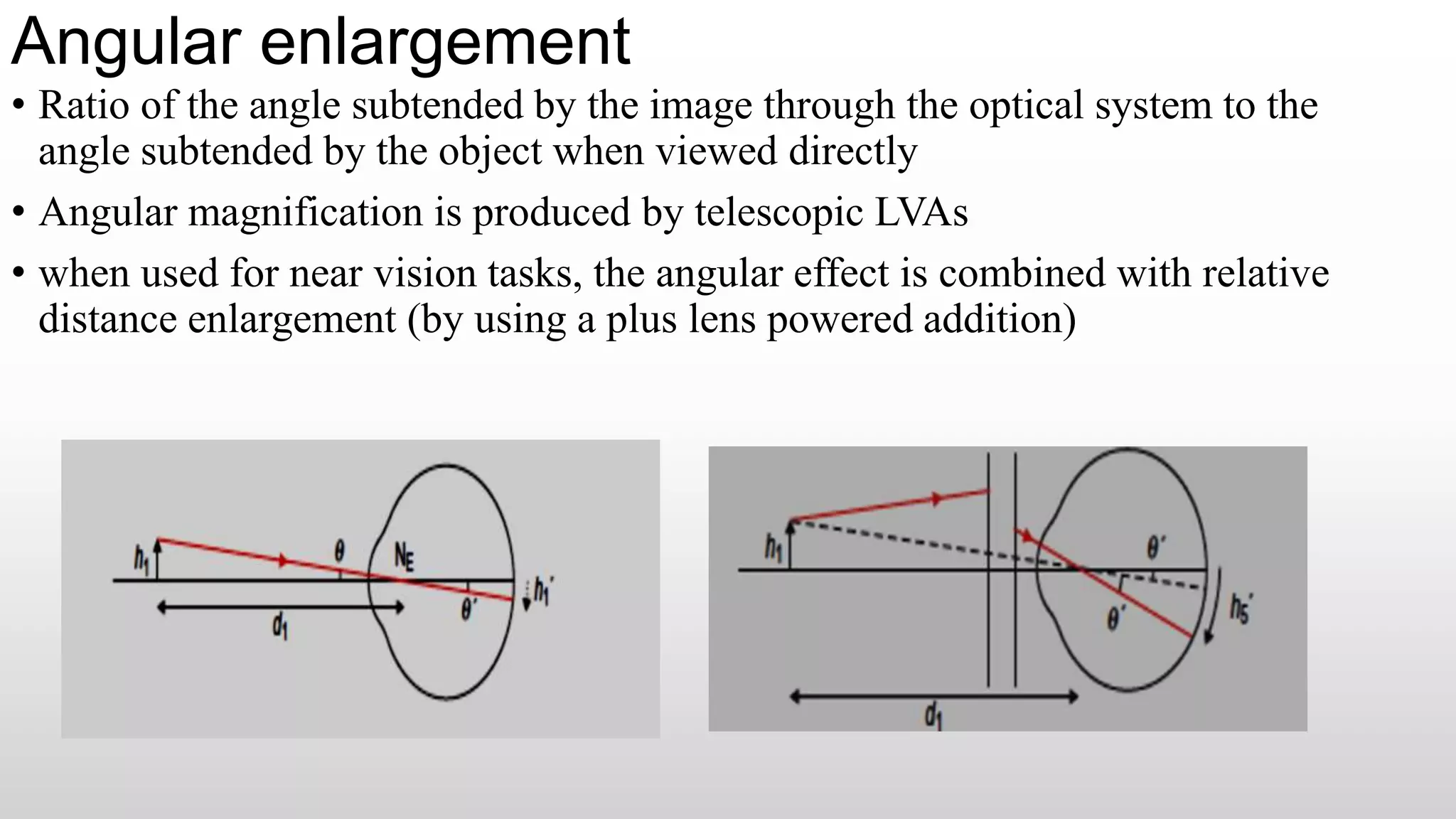
Low visual aids can be used to improve vision for those with low vision. They work by magnifying images using various optical techniques like relative distance enlargement, relative size enlargement, electronic enlargement, and angular enlargement. Common low visual aids include hand magnifiers, stand magnifiers, bar and flat-field magnifiers, spectacle magnifiers, telescopes, and electronic vision enhancement systems. Newer options include intraocular low vision aids that surgically implant a magnifying lens or retinal prosthesis inside the eye.