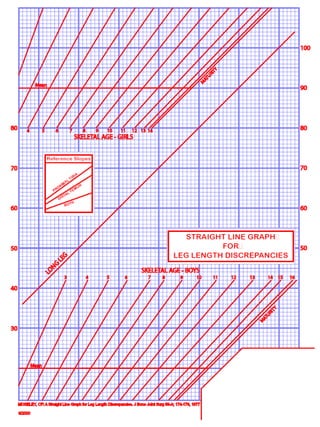
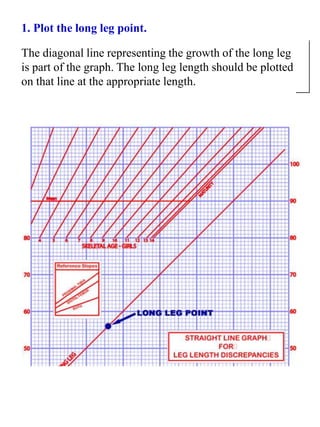
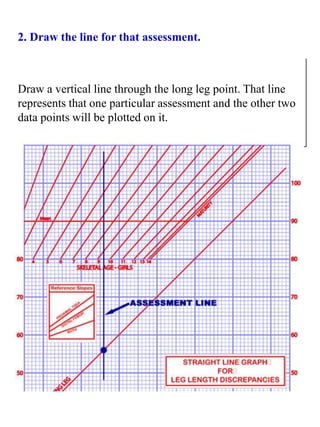
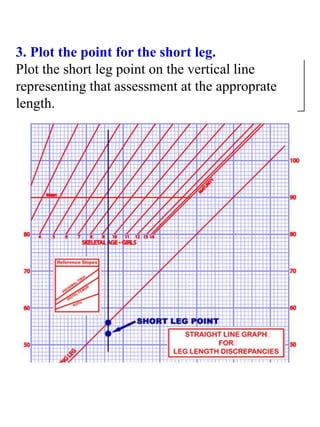
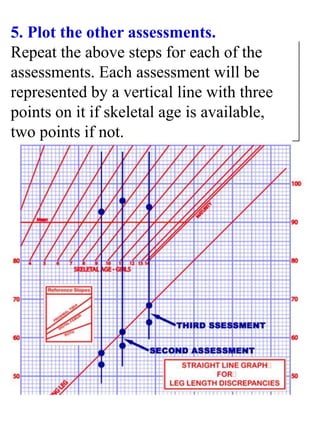
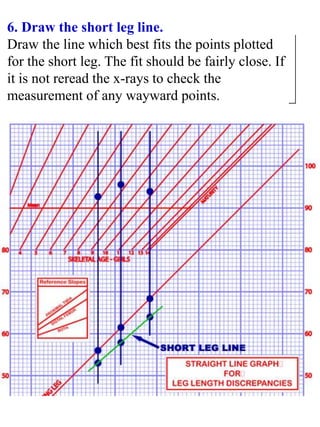
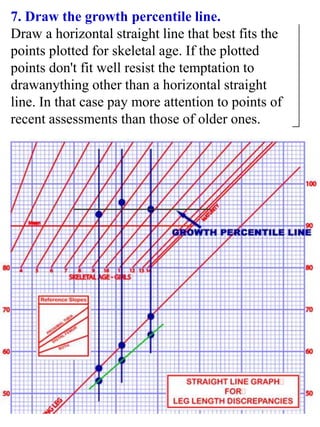
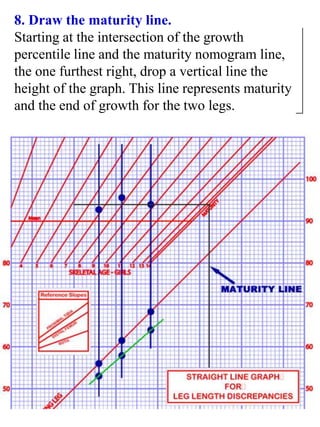
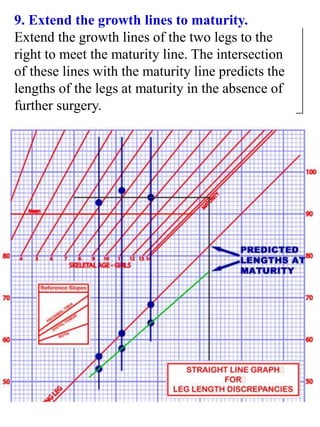
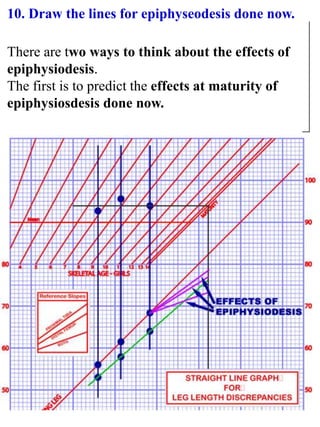
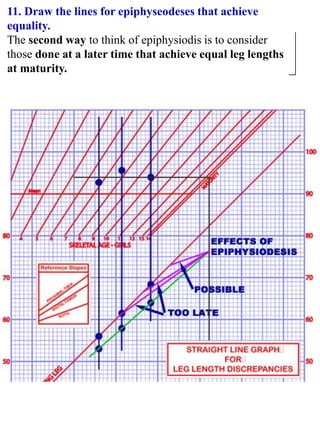
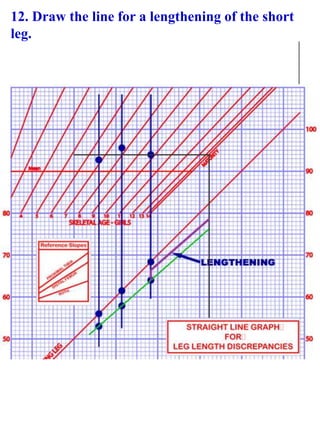
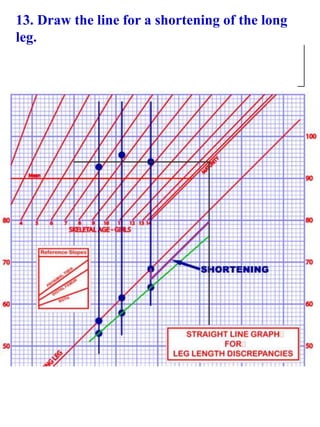
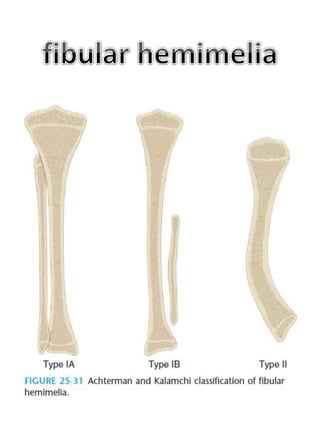
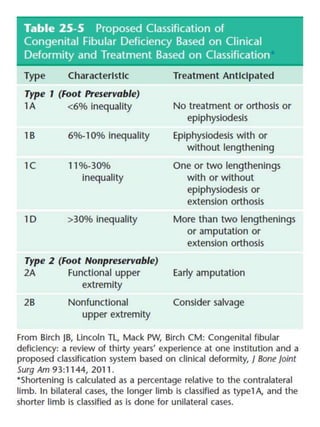
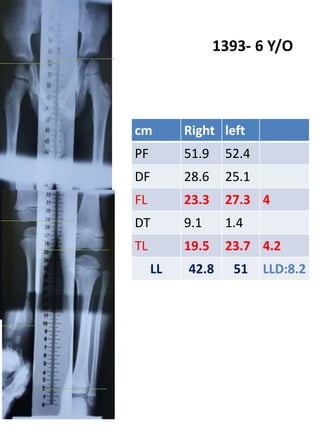
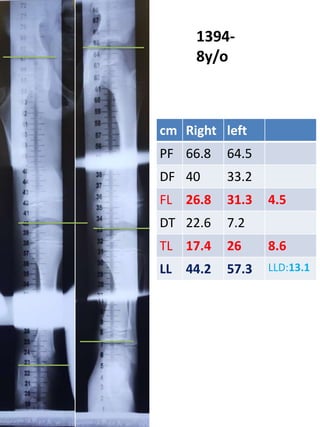
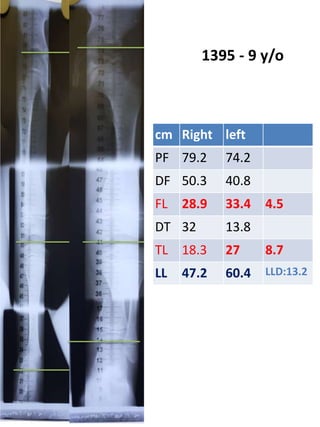
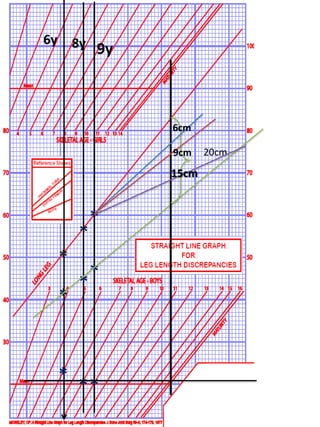
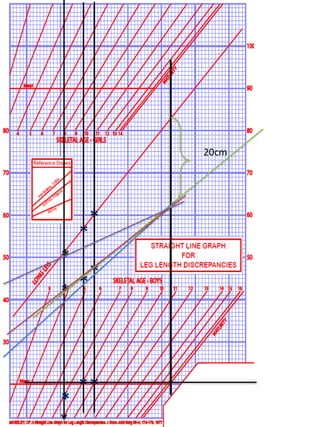
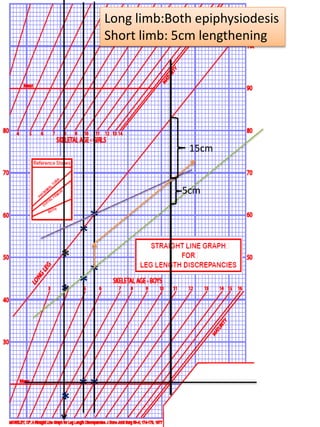
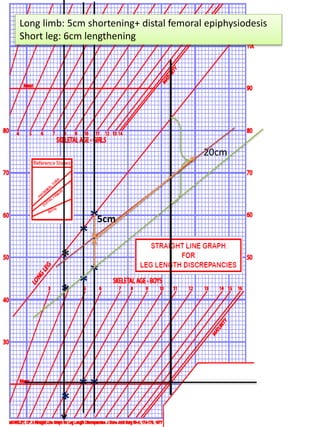
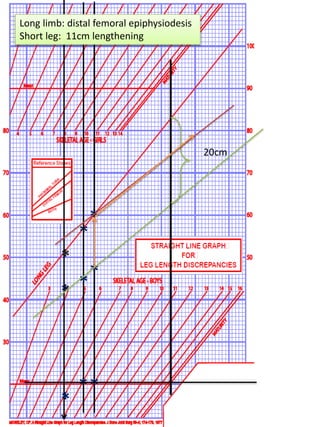
This document discusses the treatment of fibular hemimelia, a birth defect where the fibula is partially or completely absent. It describes the advantages of using the Moseley graph method to calculate leg length discrepancies and plan treatment in growing children. Treatment options discussed include amputation, limb lengthening, and epiphysiodesis (surgery to stop bone growth). For mild cases, limb lengthening may be used, while more severe cases typically require amputation. The document provides the measurements and treatment plan for a specific patient between ages 6-9 who requires epiphysiodesis and lengthening to correct their leg length discrepancy.