Anthropometry providesthe data used in the indirect
evaluation of body composition
Girths and skin folds can be entered into a number of
equations to estimate the body density, total body fat
and the overlying subcutaneous fat
trunk and limb girths provide estimates of relative
muscle mass.
Growth in statureand weight are frequently used as
markers of health, nutritional status and developmental
progress.
Both absolute and proportional changes in specific
body measures may influence strength, movement
mechanics and physiological parameters in addition to
the effects of training or detraining.
7.
The anthropometrical techniquesof proportionality
assessment can be applied to the identification of
the common physical characteristics of the athletes
within any given sport.
Within the collection of sufficient data,
anthropometrical prototypes for a certain sport can be
created. Such prototypes assist in talent
identification, training protocol and equipment
design.
1. It isnon- invasive.
2. It is relatively easy to carry out with a modest
amount of training.
3. It is possible to become skilled at acquiring
reliable measures.
4. Most techniques utilize inexpensive
equipment that is generally portable.
Growth isa major, highly variable aspect of
infancy, childhood and adolescence.
Somatic growth is more than the regular
increase of tissue mass in that it includes
dramatic alterations in size and proportion.
12.
The physique changesthat accompany growth
may affect the skill, exercise tolerance and injury
potential of an individual.
These changes can have a profound influence on
the mechanics of movement and the physiological
capacities of the growing organism.
13.
Heights and weightsare available
on specific tables of:
1. Height for age.
2. Weight for age.
3. Weight for height.
The recommended methodfor measuring the
stature is to position the subject barefoot on a level
directly against a vertical wall or door.
The subject stands erect with heels and toes together
and the arms hanging by the sides. The measurement
is taken as “the maximum distance from the floor to
the vertex of the head”
which is from the floor to the highest point on the
skull.
16.
To measurethe stretch stature, gentle upward
traction is applied from this position.
Hair clips and ribbons must be removed before the
stature is measured.
A pencil mark is made on the level of the
headboard. The subject then stands away from the
wall and the vertical distance from the floor to
the pencil mark is measured by a measuring
tape.
17.
Measuring sitting height:
“Itis the distance from vertex to the surface on
which the erect subject is seated”. There is no
consensus as to whether the feet should hang freely or
be supported
thighs should rest on a horizontal position, with knees
flexed over the edge of the sitting surface. The
subject is directed to sit up straight. Care must be
taken to ensure that the subject does not reposition
or push upwards with hands or legs
20.
Measurement is takenfrom posterior of the patient.
“The sub-ischial height (the length of the lower
limbs) is derived by subtracting sitting height from
stature height”.
21.
Measuring limb lengths:
Lengthof limb segments can be measured either
directly between two skeletal landmarks or as
vertical distance between a constant flat surface
(as the floor) and a skeletal landmark
22.
This latter ispreferred as projected lengths, which
through subtraction gives a number of derived
segment lengths (e.g. trochanteric height minus
total tibial height gives an estimate of the length of
the femur or thigh; although not accurate).
24.
The use oftape measurement is the most valid tool
for measuring limb length (long measurement).
Upper limb length discrepancy affects the
cosmetic appearance, while lower limb length
discrepancy affects both cosmetic appearance and
function.
25.
Inequality of lowerlimb length will:
1. Affect gait pattern (function).
2. Create degenerative changes in weight bearing joints.
3. Cause deformities, which may be non-structural at first,
then become structural. Unilateral shortening of lower limb
leads to pelvic tilt, scoliosis, dropping of shoulder and
tilting of head.
26.
Tape measurementis also used for
round measurement or the contour of
the:
1. Muscle to detect atrophy or hypertrophy.
2. Joint to determine swelling.
3. Chest to determine its mobility.
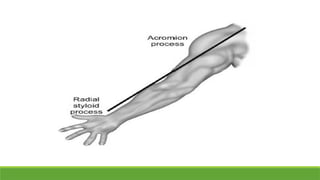
Upper limblength
Whole upper limb length: Measurement is taken
from most superior lateral point of acromion
process (acromial landmark) to the lower and
lateral border of styloid process of radius (radial
landmark).
The arm is positioned in the anatomical position,
relaxed at the side of the subject.
30.
Segmental measurement
Upper armlength: With arm flexed at 90º, so that
ulnar surface of forearm and hand are horizontal and
palms facing medially with fingers extended,
measurement is taken from acromial landmark to
the posterior surface of olecranon process of ulna.
31.
Forearm length: Itis the distance from the
head of radius (upper radial landmark) to
the most distal point of the styloid process
of radius (or styloin).
Hand length: With hand extended and the palm
rested in the direction of the longitudinal axis of
forearm, measurement is taken from styloid
process at base of thumb to the tip of middle
finger.
34.
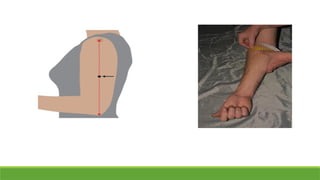
Lower limb length
Wholelower limb length: To determine true leg
length, first place the patient's legs in precisely
comparable positions and measure the distance from
the anterior superior iliac spines (ASIS) to the
medial malleoli of the ankles (from one fixed bony
point to another).
35.
Begin measurement atthe slight concavity just below
the anterior superior iliac spine, as the tape measure
may slide if pressed directly onto the spine.
If there is tilting of pelvis. Measurement will be taken
from the umbilicus to the medial or lateral malleolus.
If there is shifted umbilicus, measurement is then
taken from xyphoid process to the medial or lateral
malleolus. Apparent shortening (due to pelvic tilt)
should be differentiated from true shortening (bony).
36.
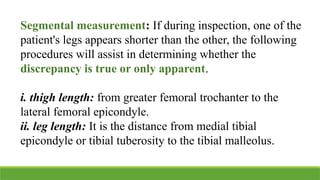
Segmental measurement: Ifduring inspection, one of the
patient's legs appears shorter than the other, the following
procedures will assist in determining whether the
discrepancy is true or only apparent.
i. thigh length: from greater femoral trochanter to the
lateral femoral epicondyle.
ii. leg length: It is the distance from medial tibial
epicondyle or tibial tuberosity to the tibial malleolus.
38.
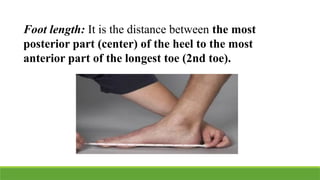
Foot length: Itis the distance between the most
posterior part (center) of the heel to the most
anterior part of the longest toe (2nd toe).
True leg lengthdiscrepancy:
Unequal distances between these fixed points verify
that one lower extremity is shorter than the other.
A true shortening may be due to
poliomyelitis or a fracture that crossed the
epiphyseal plate during childhood.
42.
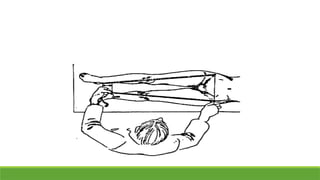
Apparent leg lengthdiscrepancy:
Before testing for apparent leg length discrepancy, no true leg
length discrepancy should be confirmed (no true bony
inequality). Apparent shortening may arise from pelvic obliquity,
hip adduction or flexion deformity.
43.
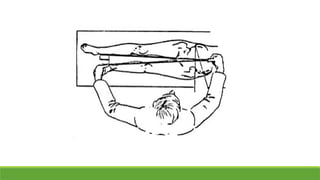
During inspection, pelvicobliquity manifests itself as uneven
ASIS or PSIS while the patient is standing.
While the patient is in supine with his legs in the neutral
position, measurement is taken from the umbilicus (or xiphi-
sternal juncture) to the medial malleolus (from a non-fixed
point to a fixed bony point). Unequal distances signify an
apparent leg length discrepancy, if the true leg length
measurements are equal.
45.
If there isan unequal limb length, the physical therapist
has to determine where the difference is via:
1. Measuring from the anterior superior iliac spine to
the greater trochanter of femur, then:
2. From the greater trochanter of femur to the lateral
articulation of the knee joint (shortening of femur).
3. From the lateral articulation of knee joint to the
medial malleolus (shortening of tibia).
46.
Quick test formeasuring lower limb length:
From crook lying position, shortening or lengthening
of femur can be detected via determining the height
of both knee joints.
Placing the two anterior superior iliac spines at the
same level shows shortening or lengthening of the
femur or tibia:
48.
1. From thelateral view: A forward projection
of knee denotes shortened tibia and
lengthened femur.
2. From the anterior view: An upward projection
of knee denotes shortened femur and lengthened
tibia.
This length islooped around the part to be
measured and held so that the printed notches on
the scale are next to each other (the
stub end is pulled superior to the easing end).
51.
As the tensionapplied to the tape varies,
skin surfaces should not be compressed or an
observable space between the skin and the tape left.
Tapes with spring easing are not recommended.
Measurements should be recorded to the nearest 0.1
cm.
52.
Head girth: Itis the maximum
circumference of the head when
the tape is located immediately
superior to the eyebrows and
positioned at the back of the head,
so that the maximum parameter is
measured.
53.
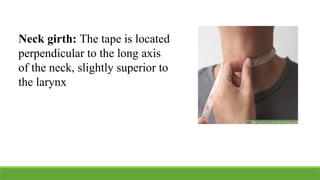
Neck girth: Thetape is located
perpendicular to the long axis
of the neck, slightly superior to
the larynx
54.
Upper limb girth
1.Mid-arm girth: It is also known as arm
circumference, upper arm circumference, biceps
circumference or relaxed arm girth. The tape is
applied around the mid-upper arm.
2. Forearm girth: This measurement is the maximal
girth of the forearm. It is taken around the upper
third of forearm
56.
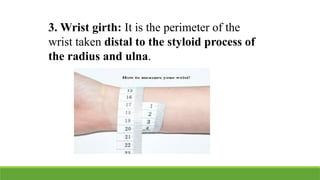
3. Wrist girth:It is the perimeter of the
wrist taken distal to the styloid process of
the radius and ulna.
57.
Trunk girth
Chest girth:The chest should be bare and the subject
stands in a natural erect posture.
Measurements are taken from under the axilla and
around the chest, passing by the xyphoid process:
- Just below the axillary fold.
- At the level of the nipple.
- At xyphoid process.
59.
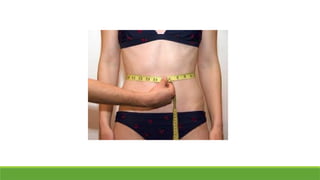
Waist girth: Itis measured at the narrowest
part of the torso.
The subject should be standing comfortably
erect with hands by the side, neither
intentionally contracting abdominal
muscles nor breath-holding.
60.
The tape isplaced aroundtorso, so that it
is snug but not compressing the skin and
the underlying tissues.
The measurements should be taken
halfway between the ribs (12th rib) and
the iliac crest.
Gluteal girth: Itis also known as the buttocks or hip
circumference. This is theperimeter at the level of the
greatest posterior protuberance of the gluteals. The
subject stands erect with minimal clothing, with the
feet together and no intentional contraction of the
gluteal muscles. The tape is placed compressing any
overlying clothing but not the soft tissues.
66.
Lower limb girth:
1.Thigh girth: It is the circumference of the thigh,
which is measured when the subject stands erect
with the legs slightly parted and his weight
distributed equally on both feet. The tape is looped
around the lower leg.
67.
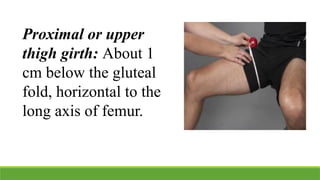
Proximal or upper
thighgirth: About 1
cm below the gluteal
fold, horizontal to the
long axis of femur.
68.
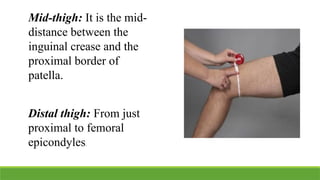
Mid-thigh: It isthe mid-
distance between the
inguinal crease and the
proximal border of
patella.
Distal thigh: From just
proximal to femoral
epicondyles.
69.
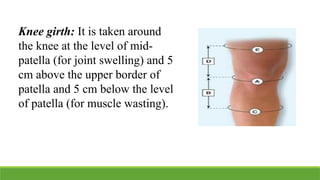
Knee girth: Itis taken around
the knee at the level of mid-
patella (for joint swelling) and 5
cm above the upper border of
patella and 5 cm below the level
of patella (for muscle wasting).
70.
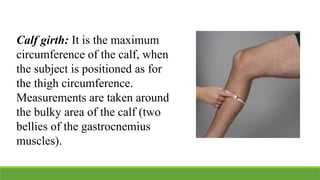
Calf girth: Itis the maximum
circumference of the calf, when
the subject is positioned as for
the thigh circumference.
Measurements are taken around
the bulky area of the calf (two
bellies of the gastrocnemius
muscles).
71.
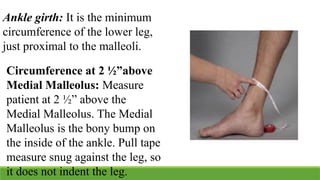
Ankle girth: Itis the minimum
circumference of the lower leg,
just proximal to the malleoli.
Circumference at 2 ½”above
Medial Malleolus: Measure
patient at 2 ½” above the
Medial Malleolus. The Medial
Malleolus is the bony bump on
the inside of the ankle. Pull tape
measure snug against the leg, so
it does not indent the leg.