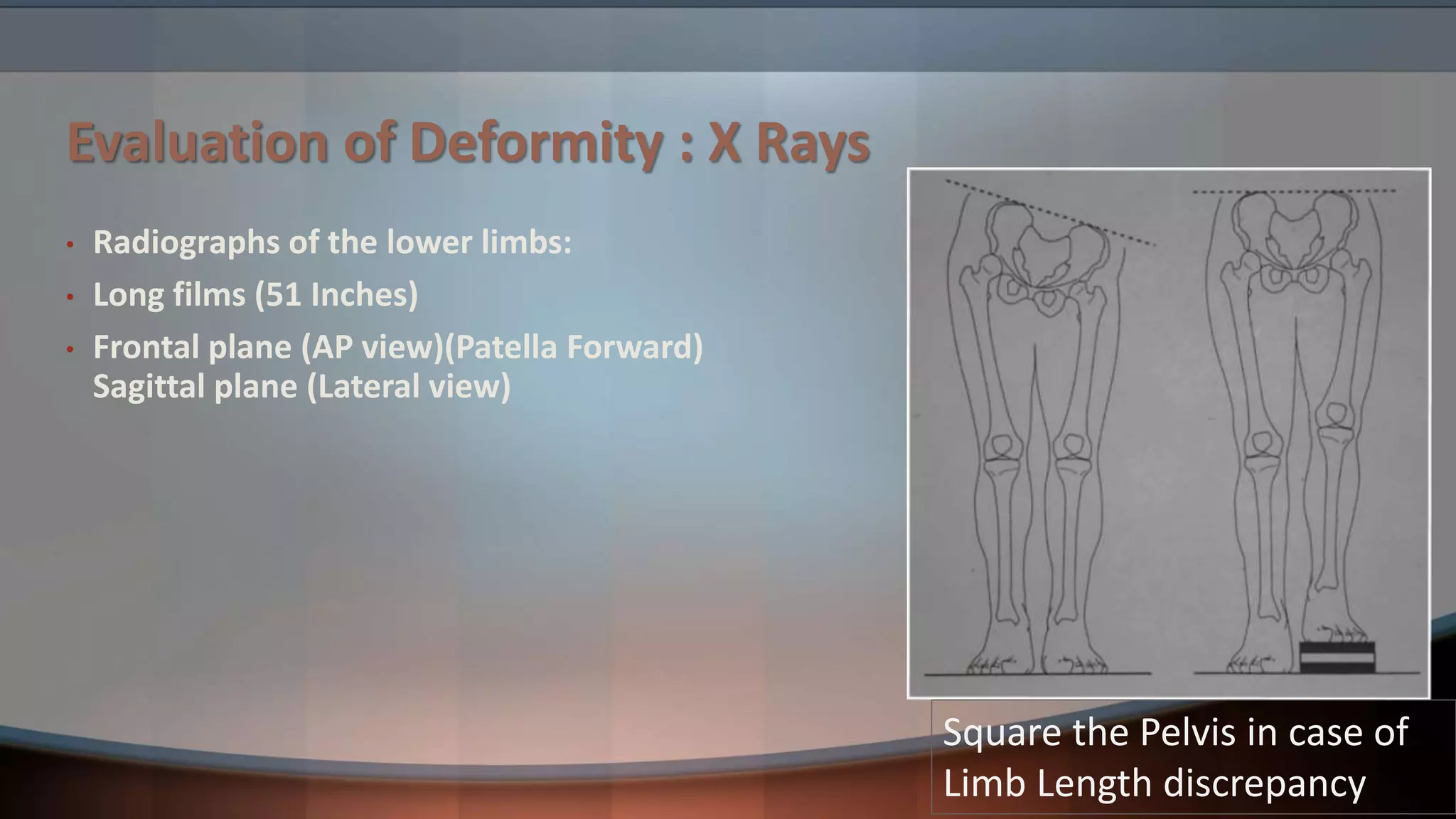
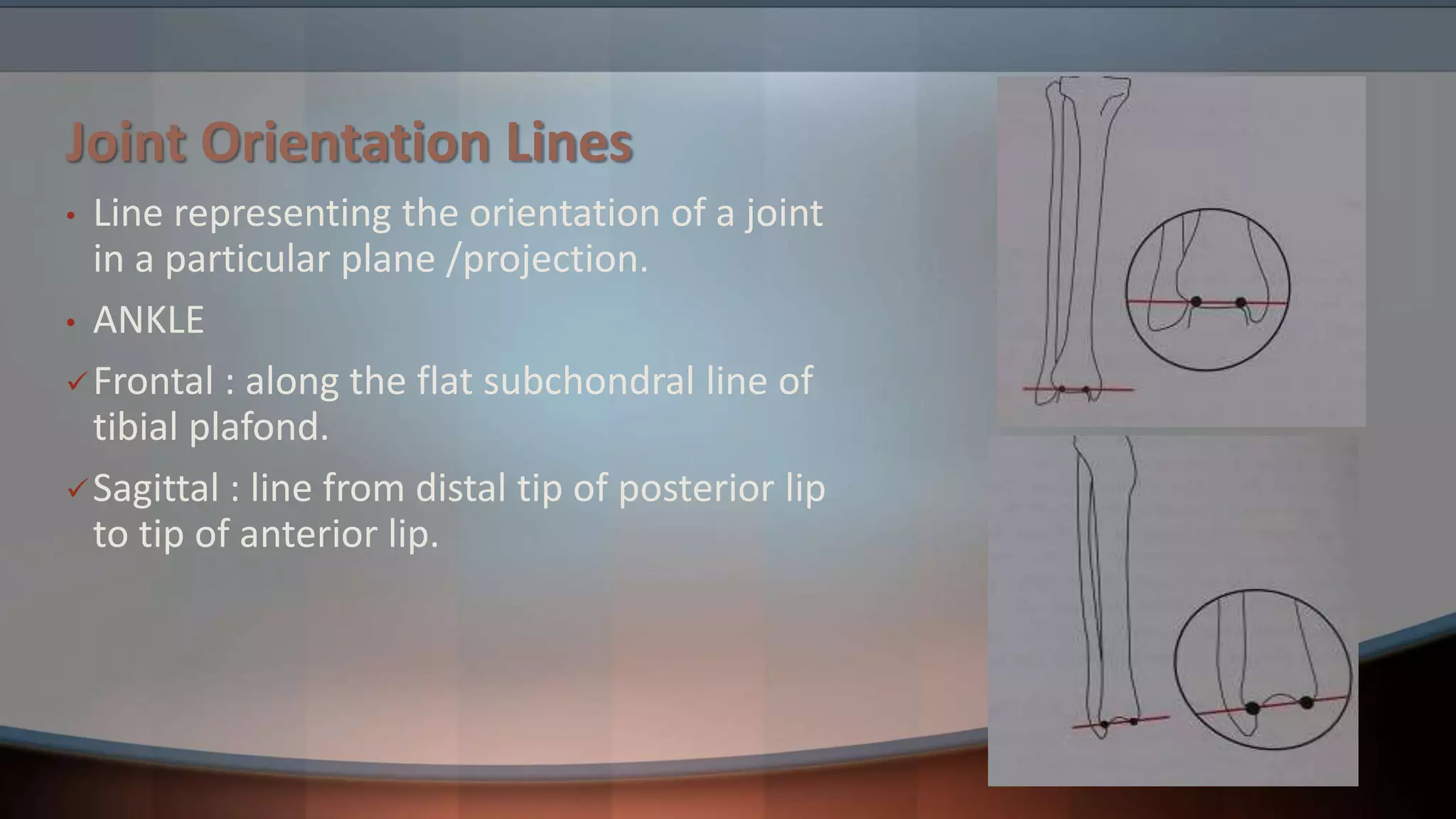
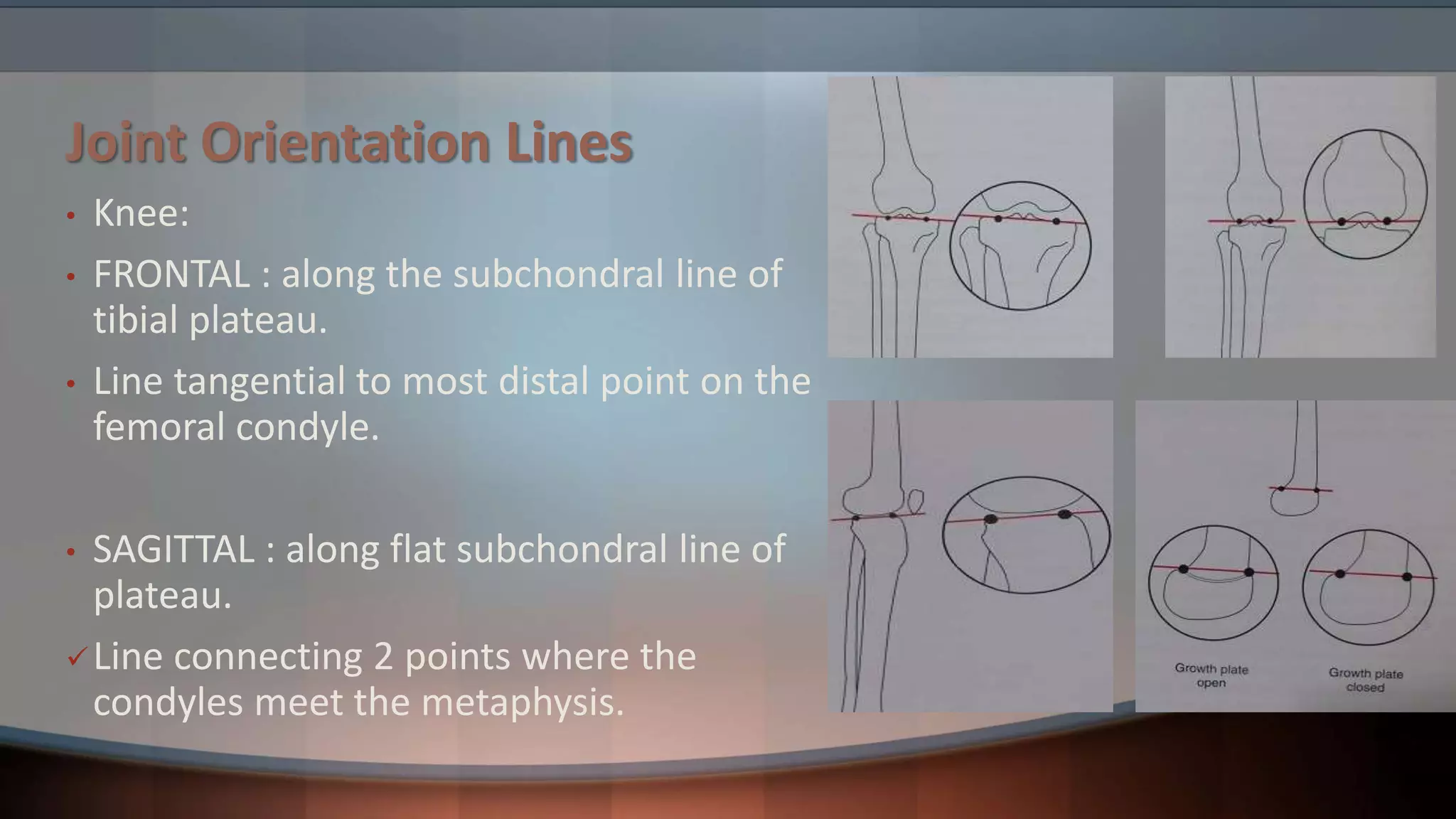
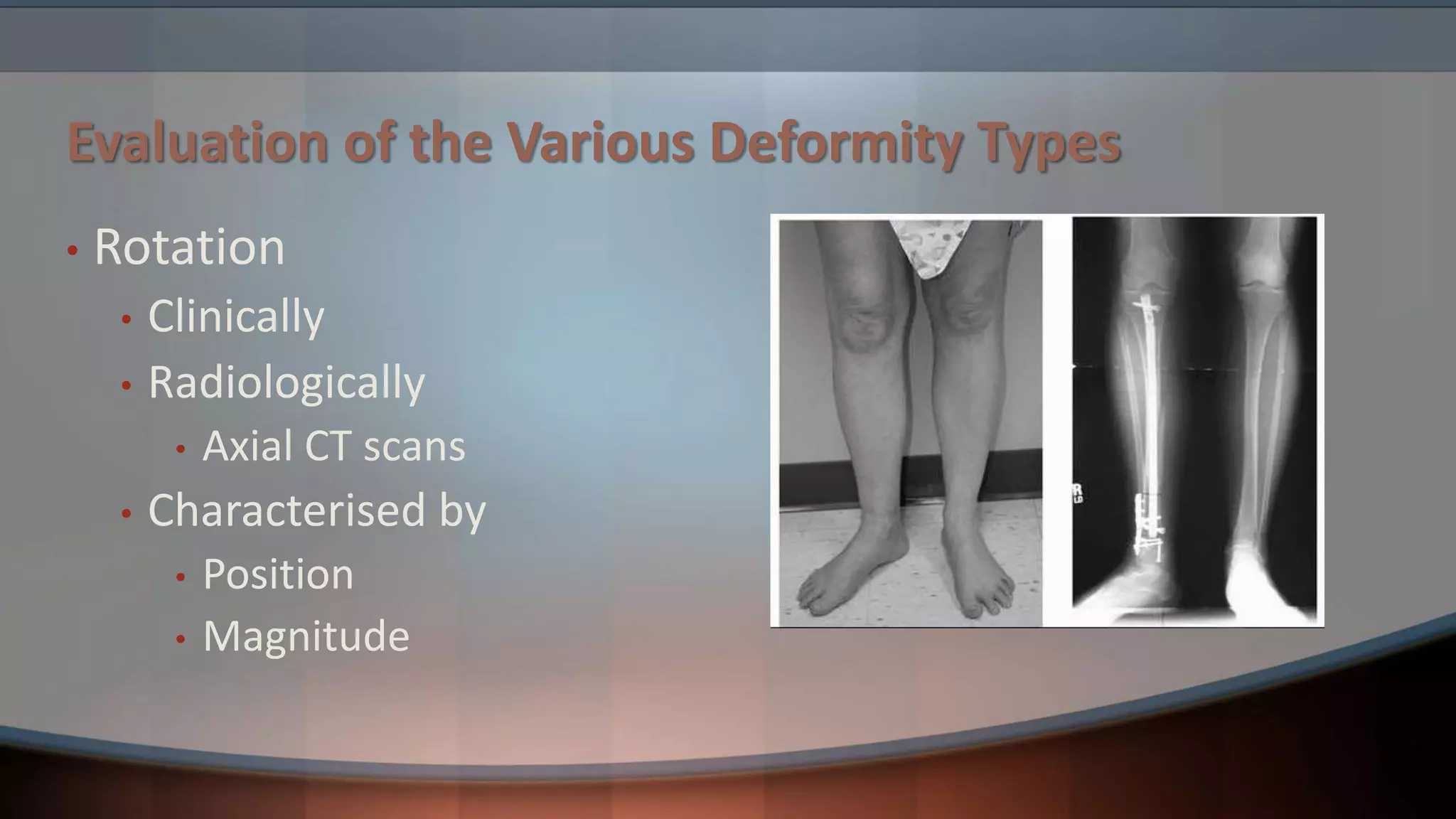
The document discusses principles of deformity correction. It defines deformity and describes how deformities are characterized by abnormalities in length, angulation, rotation, and translation. Evaluation involves clinical and radiological exams like x-rays and CT scans. Key concepts covered include mechanical and anatomical axes, joint orientation lines and angles, the center of rotation of angulation, and types of osteotomies like wedge and dome osteotomies. Treatment depends on the deformity type and involves techniques like osteotomies, external fixation, and distraction or compression to gradually or immediately correct length, angulation, rotation, and translation abnormalities.