Downloaded 111 times

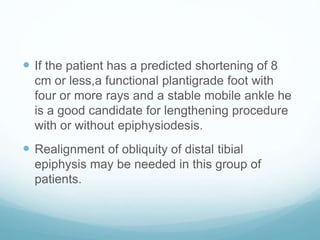
![ The limb length discrepancy with FH ranges from very
mild to very severe inhibition, ranging at maturity of the
patient from 2 to 25 cm in the absence of femoral
deficiency discrepancy. With combined inhibition of the
femur and tibia the magnitude of leg length dis-
crepancy at maturity can be [30 cm].](https://image.slidesharecdn.com/fhemimelia-170811125827/85/Fibular-Hemimelia-17-320.jpg)








Fibular deficiency, or fibular hemimelia, is a rare congenital disorder where there is partial or complete absence of the fibula bone. It can cause a range of abnormalities in the leg including limb length discrepancy, foot and ankle deformities, and knee deformities. Treatment depends on the severity of deformities and expected limb length discrepancy. For severe cases with over 25cm expected discrepancy or non-functional foot, amputation is recommended. Mild cases with functional foot may be treated with foot reconstruction and limb lengthening procedures. The goals are to manage limb length, correct bone angles, and achieve a plantigrade, painless foot.









































































