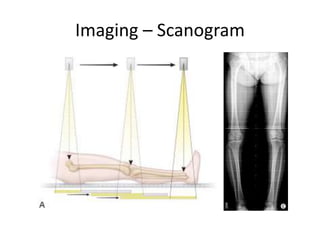
This document discusses limb length discrepancies (LLD), which occur when the paired limbs are noticeably unequal in length. It defines LLD and notes that asymptomatic discrepancies under 2cm are common. The causes, classification, evaluation, and management of LLD are described. Congenital factors, trauma, infections, and overgrowth syndromes can cause LLD. Evaluation involves history, exam, and imaging to measure the discrepancy. Management depends on the size of the discrepancy, and may include shoe lifts, epiphysiodesis, bone lengthening procedures, or amputation for large discrepancies.