Downloaded 272 times




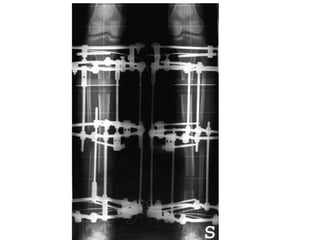




This document discusses the history and development of the Ilizarov fixator for limb lengthening. Some key points: - Previous methods from the 1940s-1960s by Anderson and Wagner were crude, requiring multiple invasive surgeries and resulting in many complications. - Soviet physician Gavriil Ilizarov in the 1940s-50s pioneered a circular external fixator made of thin wires that could gradually and safely lengthen limbs using the body's natural bone regeneration, establishing the biological principles still used today. - His method reduced complications and made limb lengthening a reliable procedure to treat many causes of limb length discrepancies and shortening.
















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
