Downloaded 2,693 times








































The document provides a comprehensive overview of heart failure, including its definition, common causes, types, pathophysiology, risk factors, signs and symptoms, diagnosis, and treatment options. It emphasizes that heart failure is a significant clinical syndrome affecting millions worldwide, primarily driven by conditions like coronary artery disease and hypertension. The management involves correcting underlying issues, nonpharmacologic therapies, and a range of medications, along with emphasizing the importance of early diagnosis and clinical evaluation.
Overview of heart failure, its definition, common causes like coronary artery disease, and global prevalence affecting millions.
Discusses leading causes of HF, types based on cardiac output, anatomical side, and onset.
Examines how heart failure affects stroke volume and compensatory mechanisms that can worsen the condition.
Identifies major risk factors for heart failure including CAD, age, hypertension, and diabetes.
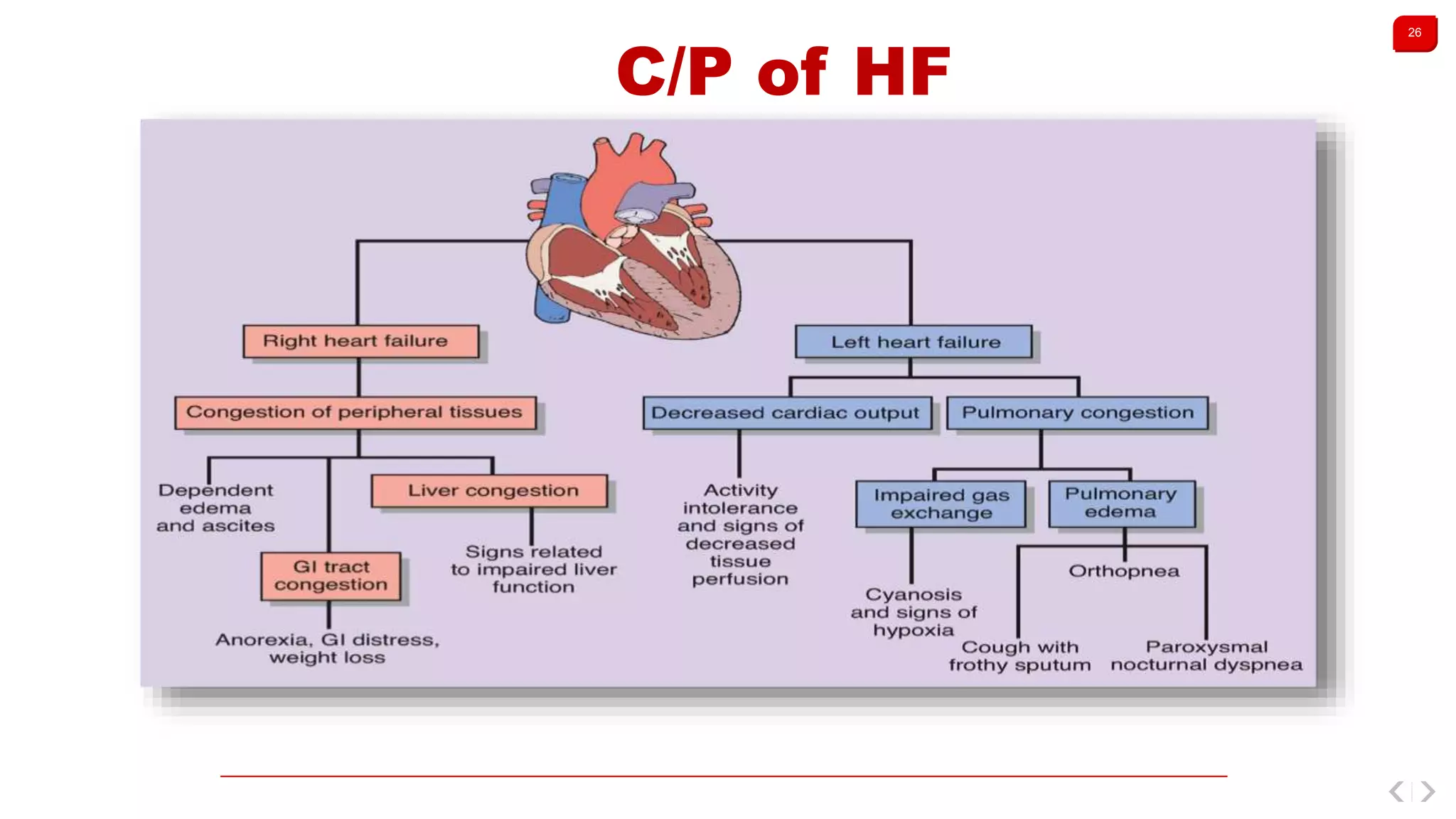
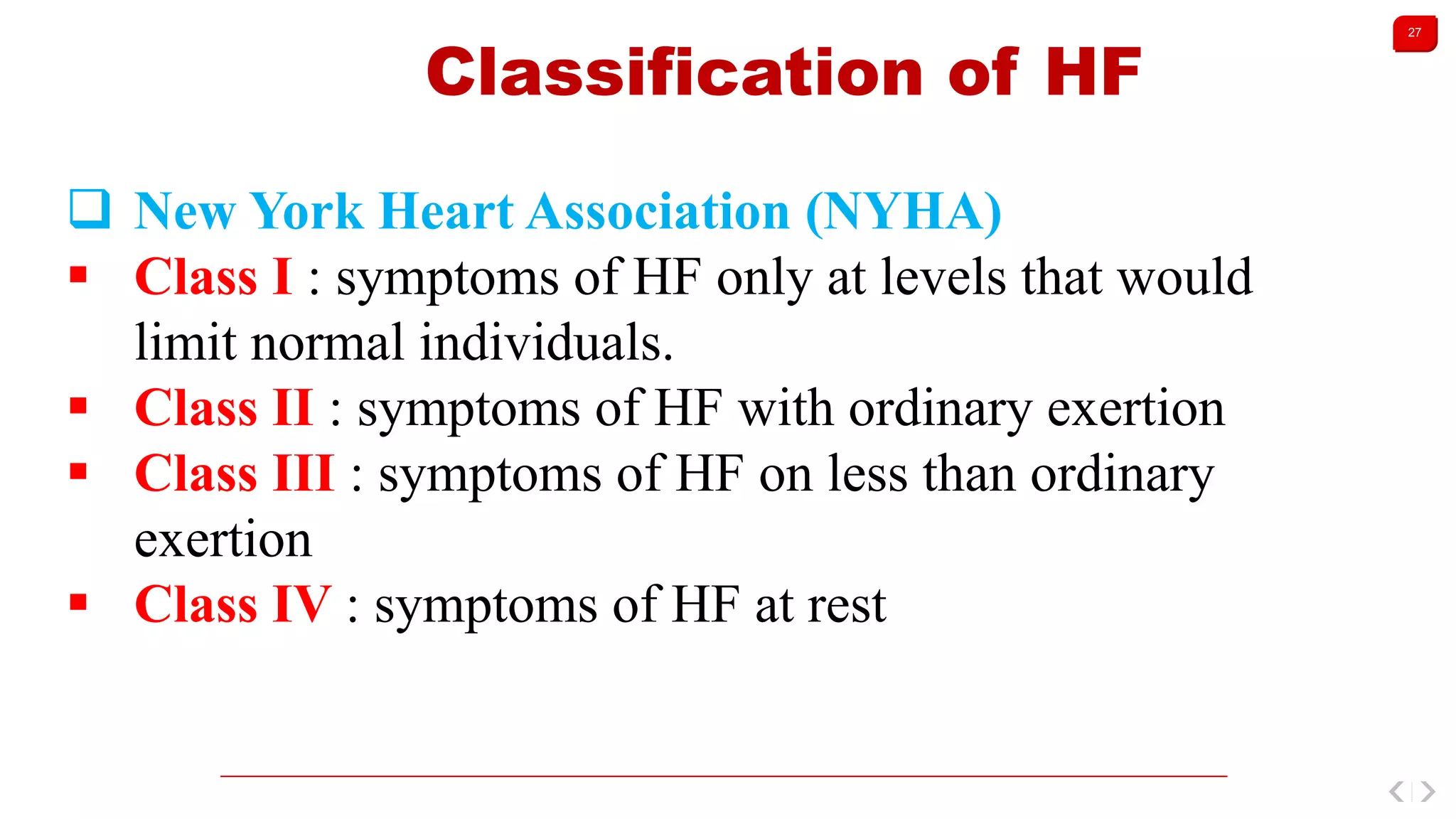
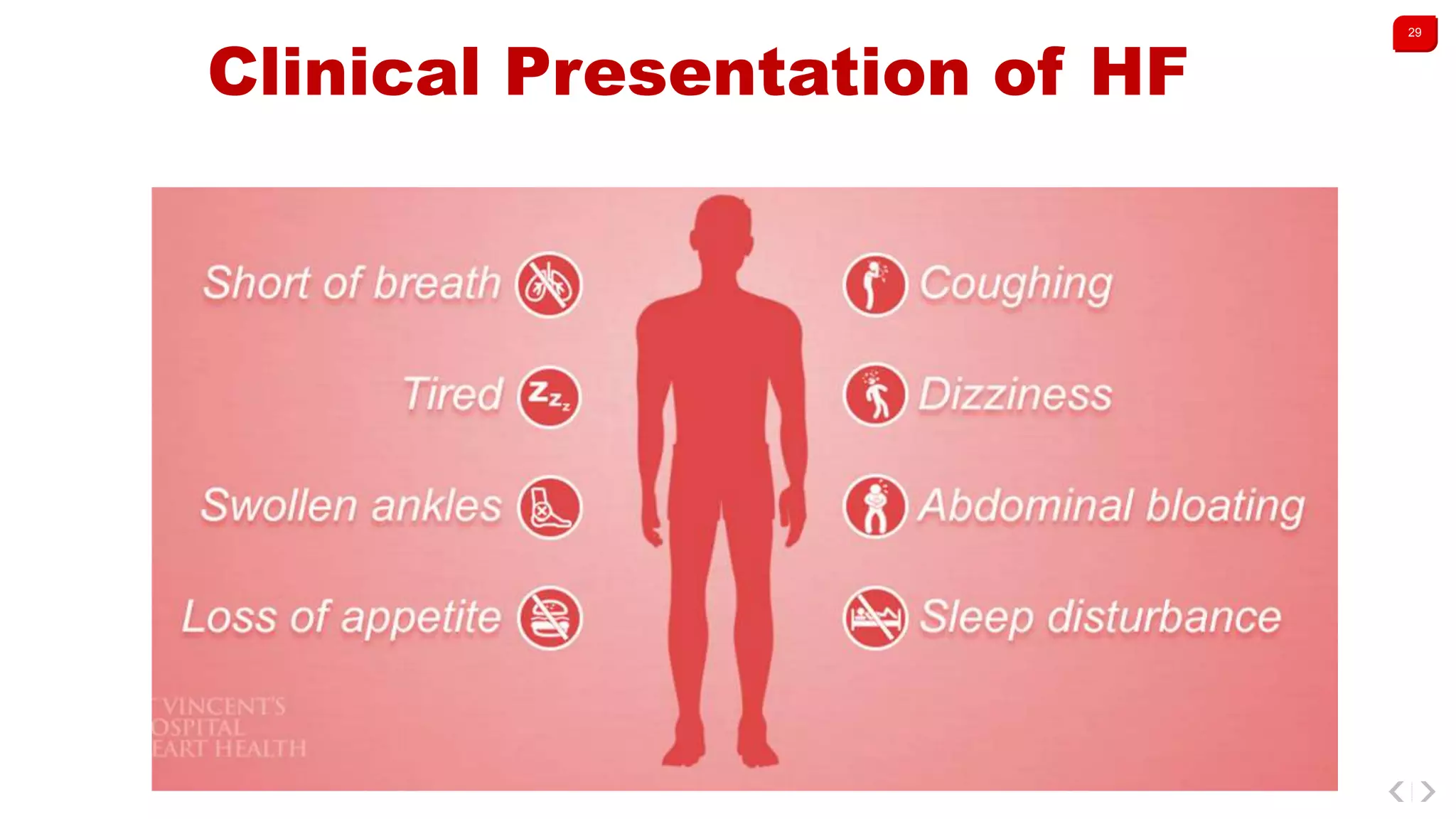
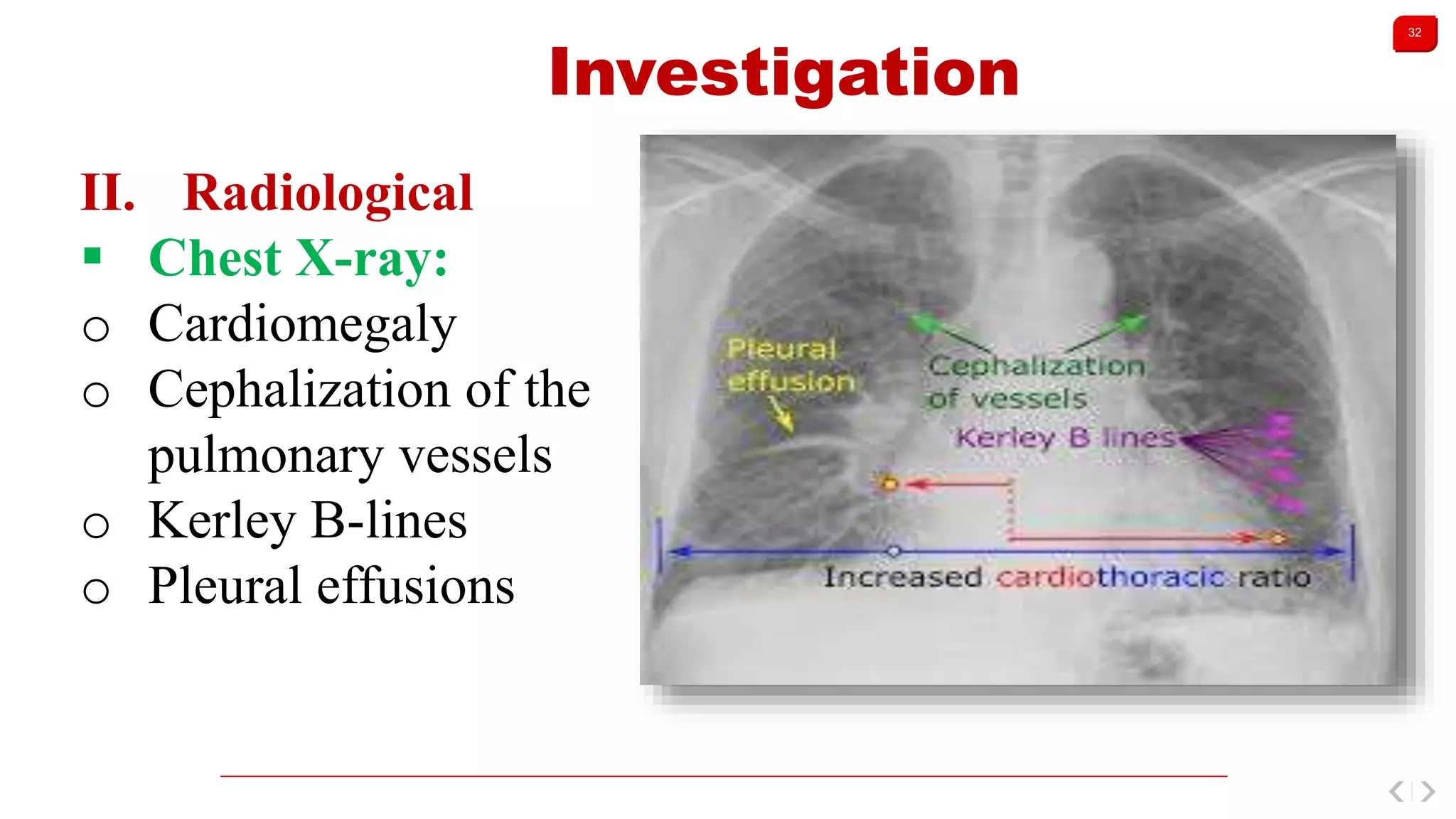
Details symptoms and signs for left and right heart failure, classification systems, and diagnostic investigations.
Management strategies, including lifestyle modifications, medical treatments, and medications to avoid.
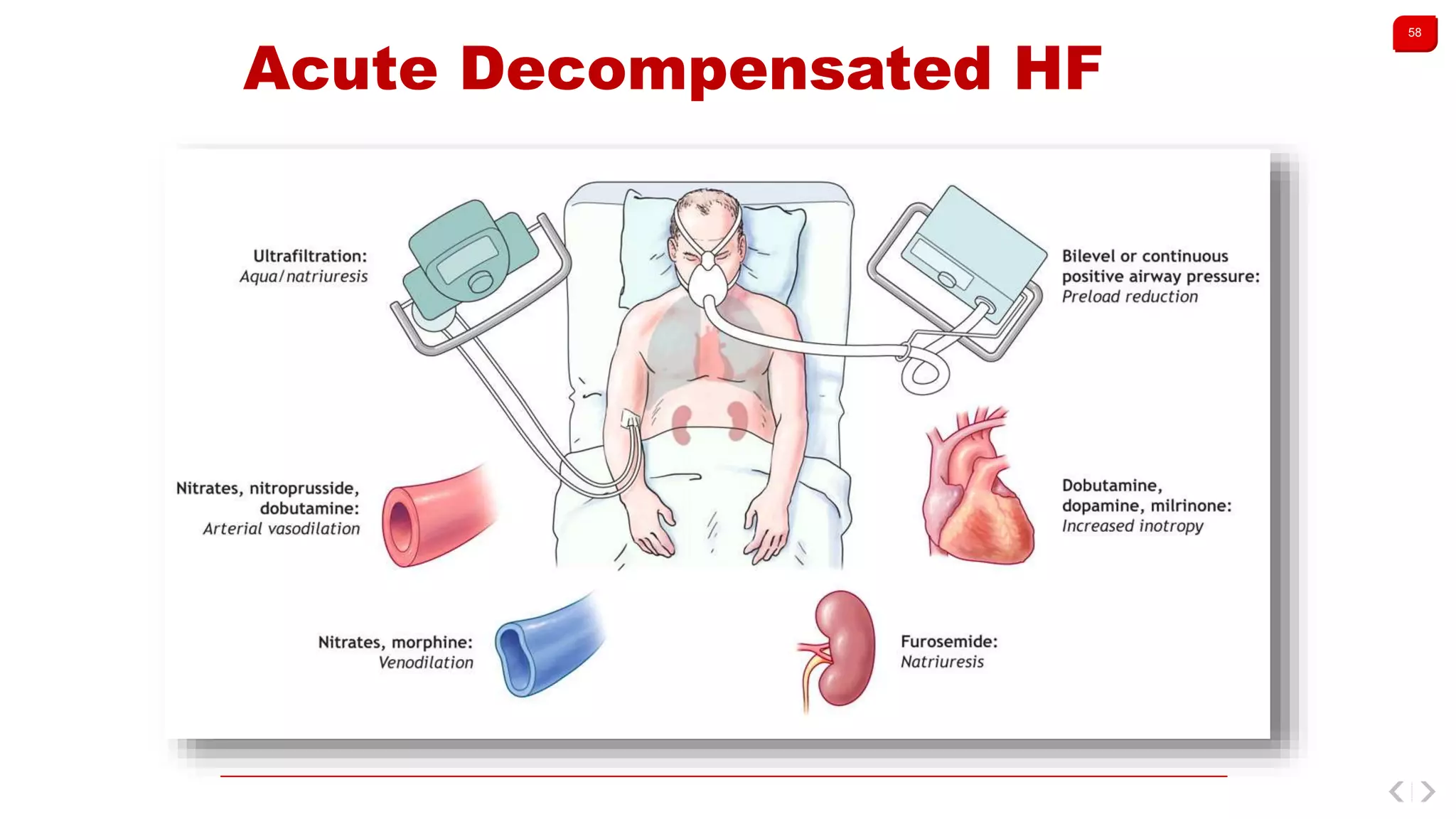
Focuses on acute decompensated heart failure, its causes, clinical manifestations, investigations, and treatment.























































































