Downloaded 260 times








![Case Scenario
• Patient M is an active woman, 70 years(1) [≈ average human life
expectancy at birth, 2011 estimate] of age, who lost consciousness
and collapsed at home. Her daughter, who was visiting her at the
time, did not witness the collapse but found her mother on the floor,
awake, confused, and slightly short of breath. The daughter estimated
that she called EMS within 5 minutes after the collapse, and EMS
responded within 10 minutes. EMS evaluated Patient M, drew blood
for a glucose level, and determined that she may have had a stroke.
They notified the nearest designated comprehensive stroke center
that they would be arriving with the patient within15 minutes(1).
Patient M's daughter accompanied her.](https://image.slidesharecdn.com/cerebrovasculardisease-161207034747/85/Cerebrovascular-disease-22-320.jpg)


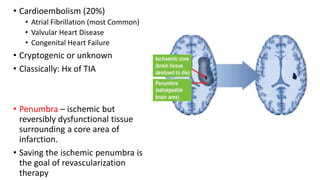
1. A 70-year-old woman collapsed at home and was found confused by her daughter. EMS determined she may have had a stroke and transported her to the hospital within 30 minutes of the collapse. 2. At the hospital, she was found to have high blood pressure, left-sided weakness, and a CT scan showed a blood clot in her carotid artery causing a right hemisphere stroke. 3. Her risk factors included a history of untreated hypertension and a previous transient ischemic attack. She was diagnosed with an ischemic stroke likely due to atherosclerosis.





























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















