Downloaded 77 times

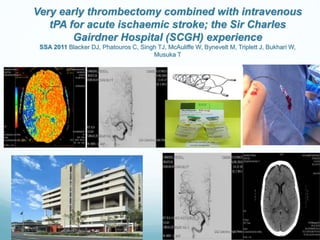



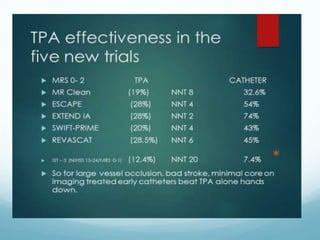
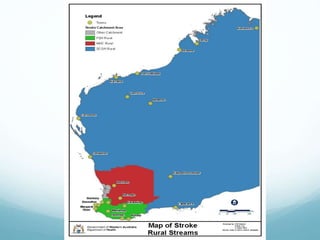



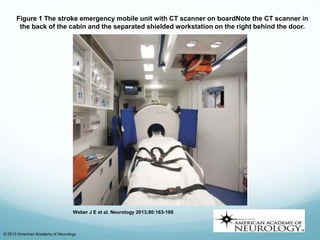







1) Minocycline, a tetracycline antibiotic, may reduce hemorrhagic transformation after acute ischemic stroke when given intravenously with tPA. 2) Endovascular approaches such as intra-arterial thrombolysis and thrombectomy are promising options for treating large vessel occlusions in acute ischemic stroke beyond the current treatment window of 4.5 hours. 3) Pre-hospital administration of therapies such as magnesium may expand the treatment window for acute ischemic stroke if given soon after symptom onset in the field before hospital arrival.





































































































