


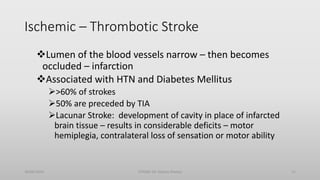

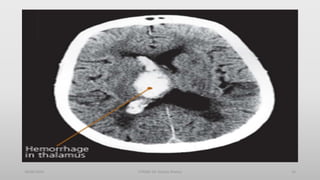






This document discusses stroke, including defining it as resulting from ischemia or hemorrhage in the brain, listing common risk factors like age, hypertension and diabetes, classifying strokes as ischemic or hemorrhagic, and describing diagnostic tools like CT scans and MRI. Ischemic strokes are further divided into thrombotic and embolic types while hemorrhagic strokes are intracerebral or subarachnoid. Clinical effects and sites of pathology are outlined for different stroke types.



















































![Applied Anatomy &Physiology of Cranial nerves [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/appliedanatomyphysiologyofcranialnervesautosaved-250912155808-c3374f2c-thumbnail.jpg?width=640&height=640&fit=bounds)




















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









