
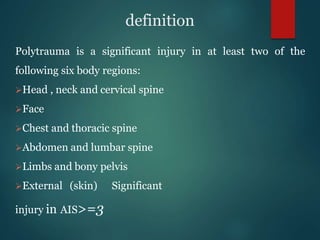

















































Polytrauma refers to significant injuries across two or more body regions, leading to various types of shock and requiring immediate and comprehensive trauma care. Management involves rapid assessment, resuscitation, and definitive care within critical time frames, particularly the 'golden hour' post-injury. Common causes include vehicle accidents, falls, and assaults, with the condition posing substantial mortality risks and necessitating a coordinated medical response from emergency services to hospital staff.































![Approach_to_the_trauma_patient[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtothetraumapatient1-220906191256-c4d92395-thumbnail.jpg?width=640&height=640&fit=bounds)


















































