Downloaded 255 times


























![PULMONARY FUNCTION TEST
Optimal candidates are those with severe obstructive
disease (forced expiratory volume in one second [FEV1]
<40% predicted) without a significant restrictive component
or reversible bronchoconstriction.
Plethysmography must demonstrate significantly increased
total lung capacity (TLC) >120% predicted as well as
elevated residual volume (RV) >150% predicted.
Initial testing also includes determination of resting arterial
blood gases (PO2 and PCO2). The diffusing capacity (DLCO)
is also measured and, proves to be an important parameter
that can occasionally contraindicate surgical intervention.
Ideally, patients who are candidates for LVR have a PO2
>60, a PCO2 <55 mm Hg, and a DLCO >20% predicted.](https://image.slidesharecdn.com/lungvolumereductionsurgery-140504024505-phpapp02/75/Lung-volume-reduction-surgery-31-2048.jpg)












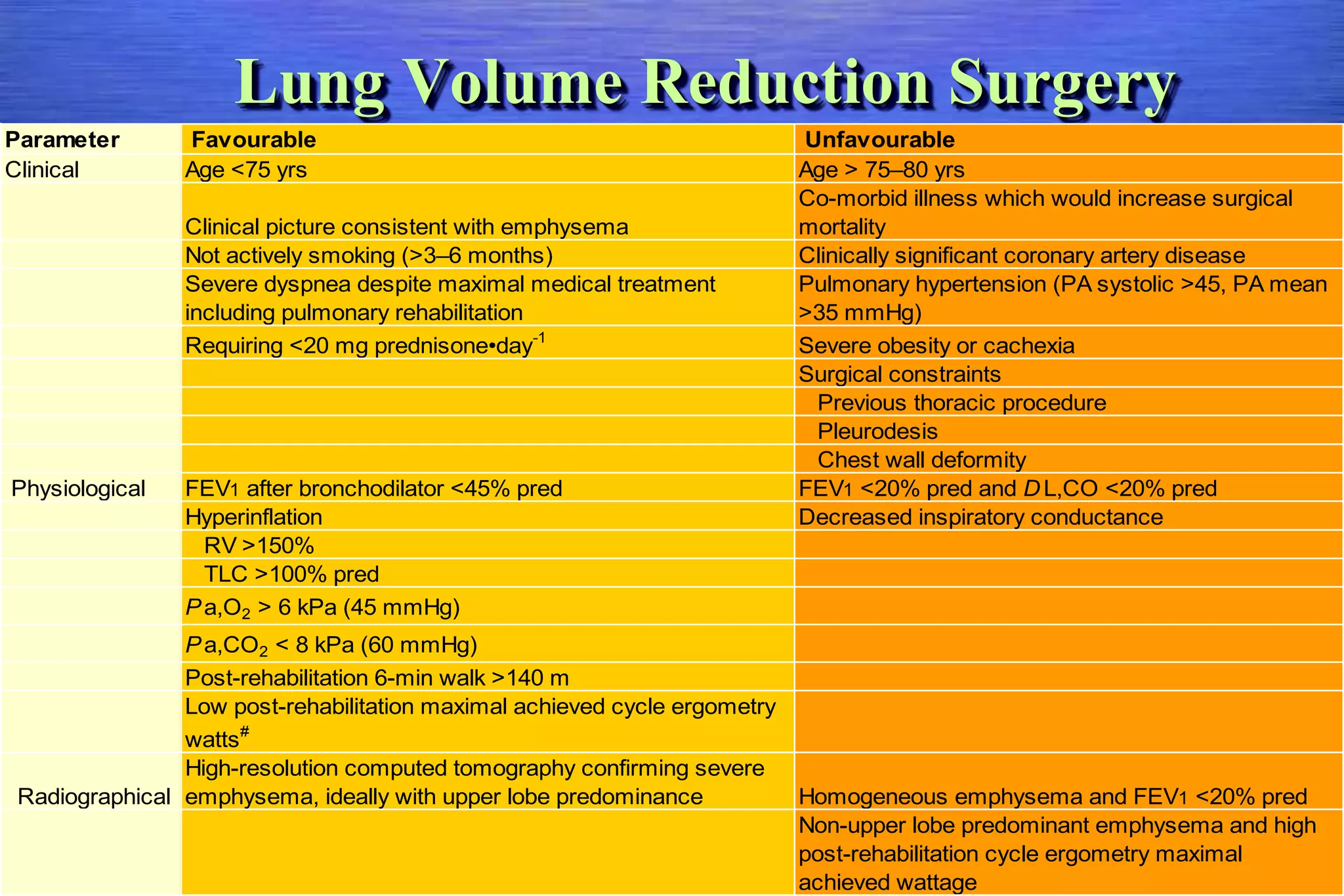

































LVRS involves surgically removing portions of emphysematous lung to allow the remaining lung tissue to expand. The NETT trial found LVRS benefits patients with upper lobe-predominant emphysema and low exercise capacity by improving lung function, exercise ability, and quality of life. Candidates for LVRS have severe emphysema, poor exercise capacity, marked lung hyperinflation, and meet criteria for pulmonary function tests, exercise testing, and cardiac/pulmonary evaluations. The procedure aims to improve ventilation/perfusion matching, reduce airway resistance, and allow the chest wall and diaphragm to resume a more normal position.











































































































