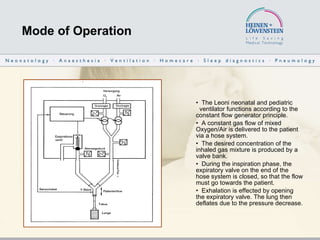
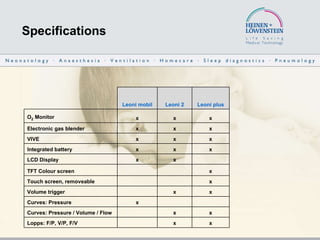
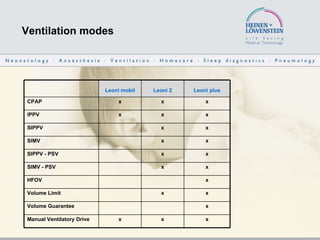
The document describes the Leoni series of neonatal and pediatric ventilators produced by Heinen + Löwenstein GmbH. It provides details on the operation, specifications, ventilation modes, settings, components, accessories, and total system of the Leoni plus, Leoni 2, and Leoni mobil ventilators. High-frequency oscillatory ventilation is discussed as an option for treatment of lung diseases with reduced compliance.


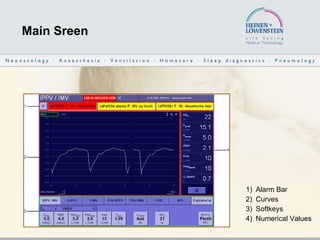
![Setting ranges IPPV/ IMV SIMV SIPPV CPAP Breath rate FREQUENCY [BPM] 6 .. 200 2 .. 100 2 .. 100 - Inspiration time I-TIME [sec] 0.10 .. 2.00 0.10 .. 2.00 0.10 .. 2.00 - Expiration time E-time [sec] 0.20 .. 10.00 0.50 .. 30.00 0.20 .. 30.00 - Inspiratory Flow INSP FLOW [l/min] 1 .. 32 1 .. 32 1 .. 32 - Expiratory Flow E Flow [l/min] 2 .. 10 2 .. 10 2 .. 10 -](https://image.slidesharecdn.com/leoniplusprsenthfoeng-12541049364362-phpapp02/85/Leoni-Plus-PraSent-Hfo-Eng-14-320.jpg)
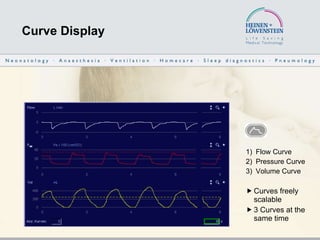
![Setting ranges IPPV/ IMV SIMV SIPPV CPAP Inspiratory Pressure P INSP [cmH2O] 6 .. 60 6 .. 60 6 .. 60 - Backup Pressure P-BACK [cmH2O] - - - 6 .. 60 Positive End Expiratory Pressure PEEP [cmH2O] 0 .. 20 0 .. 20 0 .. 20 - CPAP [cmH2O] - - - 1 .. 20](https://image.slidesharecdn.com/leoniplusprsenthfoeng-12541049364362-phpapp02/85/Leoni-Plus-PraSent-Hfo-Eng-15-320.jpg)
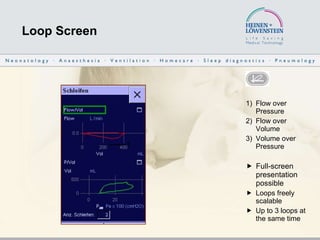
![Setting ranges IPPV/ IMV SIMV SIPPV CPAP O 2 Concentration OXYGEN [%] 21 .. 100 21 .. 100 21 .. 100 21 .. 100 O 2 Concentration Oxygen flush O2-Flush [%] 23 .. 100 23 .. 100 23 .. 100 23 .. 100 Volume trigger TRIGGER [% VTi] - 10 .. 30 10 .. 30 -](https://image.slidesharecdn.com/leoniplusprsenthfoeng-12541049364362-phpapp02/85/Leoni-Plus-PraSent-Hfo-Eng-16-320.jpg)
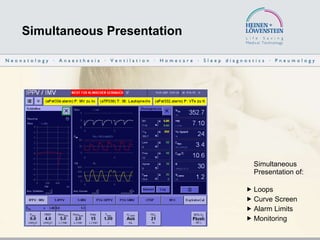
![Setting ranges HFOV Mean Pressure Pmean [cmH2O] 10 .. 30 High Frequency HFFreq [Hz] 5 .. 20 High Frequency Amplitude HFAmpl [cmH2O] 5 .. 80 Recruitment Frequency FreqRec [1/min] 0 .. 10 Recruitment Inspiration Time TI Rec [s] 0.1 .. 3](https://image.slidesharecdn.com/leoniplusprsenthfoeng-12541049364362-phpapp02/85/Leoni-Plus-PraSent-Hfo-Eng-17-320.jpg)










































![Conferencia reforma laboral febrero 2012 eada (1) [modo de compatibilidad]](https://cdn.slidesharecdn.com/ss_thumbnails/conferenciareformalaboralfebrero2012eada1mododecompatibilidad-120228064334-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




























