Downloaded 167 times

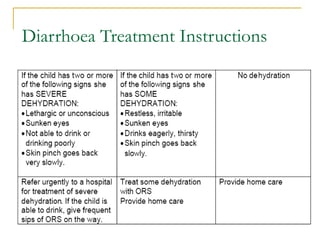
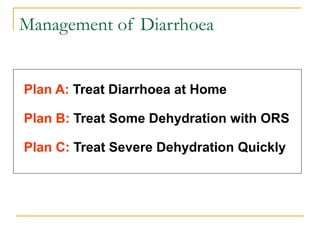
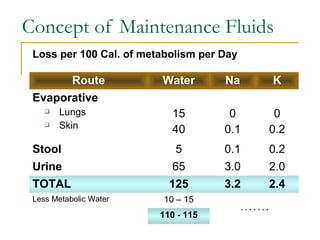
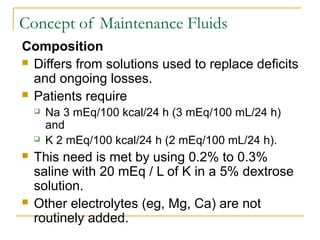
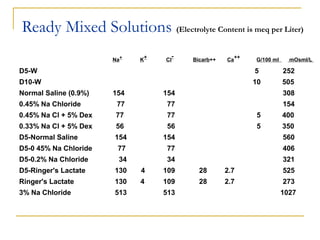
![Concept of Maintenance Fluids
Calculation based on caloric expenditure
[ Holiday & Segar Formula ]
Wt. Calories Expended Maintenance waterWt. Calories Expended Maintenance water
Till 10 Kg 100 Cal / Kg 100 ml / Kg
10 – 20 Kg 1000 Cal + 50 Cal for 1000 ml + 50 ml for
Every Kg > 10 / Kg Every Kg >10 / Kg
20 Kg 1500 Cal + 20 Cal for 1500 ml + 20 ml for
every Kg above 20 Kg every Kg above 20 Kg](https://image.slidesharecdn.com/fluidtherapy-140530040448-phpapp02/85/Fluid-therapy-46-320.jpg)
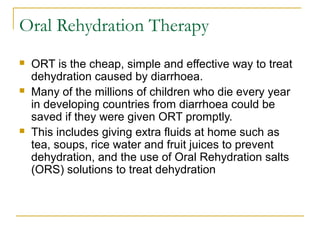
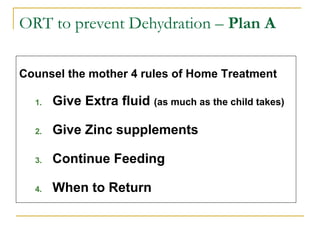
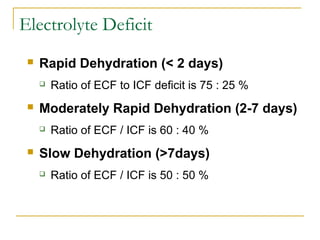
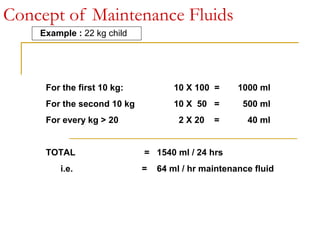
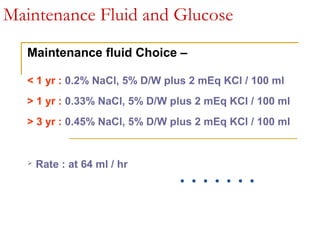
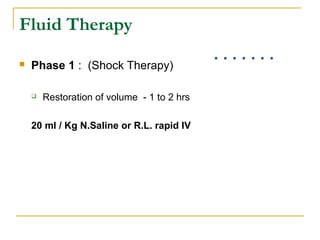
![Concept of Maintenance Fluids
Calculation based on caloric expenditure
[ Holiday & Segar Formula ]
Wt Water (ml /day) Water
ml / hr
Electrolytes
mEq / L of water
0 – 10 kg 100 ml / kg 4 / kg Na 30, K 20
10 – 20 kg 1000 + 50 ml /kg for
each kg above 10
40 + 2 / kg
for each kg
above 10
Na 30, K 20
> 20 kg 1500 + 20 ml /kg for
each kg above 20
60 + 1 / kg
for each kg
above 10
Na 30, K 20
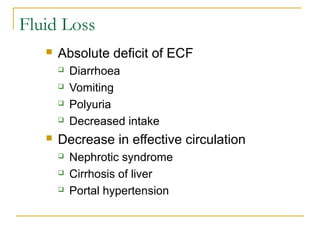
Baseline estimates are affected by fever (increasing by 12% for each degree
> 37.8° C), hypothermia, and activity (eg, increased for hyperthyroidism or
status epilepticus, decreased for coma).](https://image.slidesharecdn.com/fluidtherapy-140530040448-phpapp02/85/Fluid-therapy-48-320.jpg)
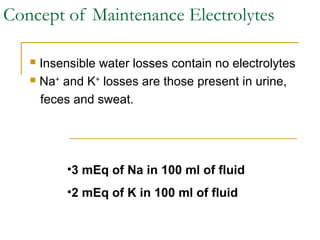
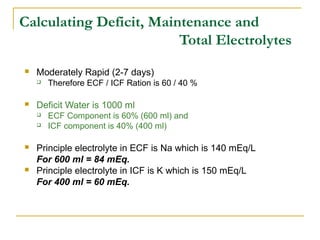
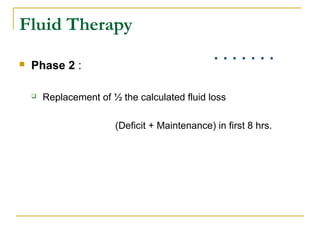
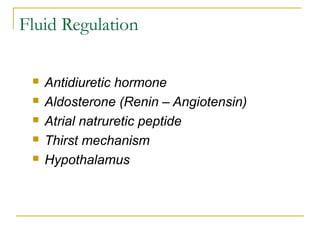
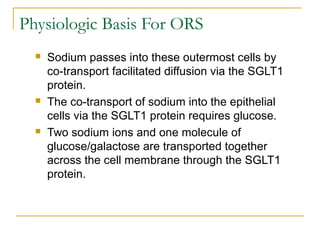
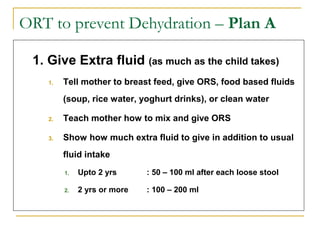
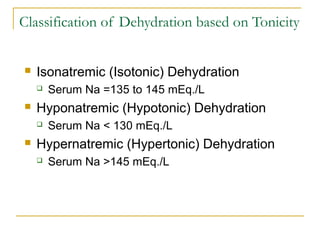
![Eg. 10 Kg child
Phase 1 (1st
hr)
20 ml / Kg of NS
(200 ml of NS, 31 mEq. of Na)
Phase 2 (2-8 hrs)
Replace half the fluid loss in next 7 hrs
900 ml in 7 hrs That is 129 ml / hr
We like to add Na in a conc of 46 mEq. L
(which is roughly in 1/3rd
NS
We can use 1/3 NS in 5% D/W at 129 ml / hr.
Phase 3 (hrs. 9-24) [ patient voids ]
Replace remaining half of fluid loss and add K now
900 ml over 16 hrs of D5, 1/3 NS at 56ml/hr
(Pt has 25mEq/L of K loss. We are replacing 900 ml (roughly 1 L) of
fluid we may chose 25mEq./L of KCl](https://image.slidesharecdn.com/fluidtherapy-140530040448-phpapp02/85/Fluid-therapy-61-320.jpg)

This document discusses fluid and electrolyte therapy. It covers the components of body water, body fluid composition, electrolyte balance, water content at different ages, regulation of body water and electrolytes, dehydration, and oral and intravenous fluid therapy. Some key points include: - Body water is divided into extracellular fluid (ECF) and intracellular fluid (ICF) - Electrolytes like sodium, potassium, and chloride are important for fluid balance and cell function - Dehydration occurs when fluid losses exceed intake and can be classified as mild, moderate, or severe - Oral rehydration therapy (ORT) using oral rehydration salts (ORS) is the main treatment for dehydr











































































































