Downloaded 414 times


![Hypernatremic Dehydration
Fluid deficit =
• Replace with D50.2%NS
• Replace over 48hrs
• Reduce sodium by no more than 10mEq/L/24hrs
Water deficit (in L) = [(current Na level in mEq/L ÷ 145
mEq/L) - 1] X 0.6 X weight (in kg)
(½ deficit – the bolus) over the first 24hrs
Add maintenance and any ongoing losses to above
Further ½ the deficit replaced over the next 24hrs](https://image.slidesharecdn.com/dehydratoninpediatrics-131005021152-phpapp01/85/Dehydraton-in-pediatrics-52-320.jpg)
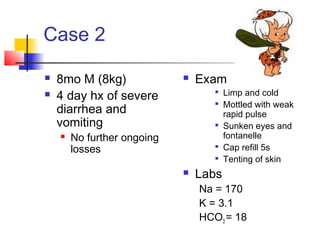

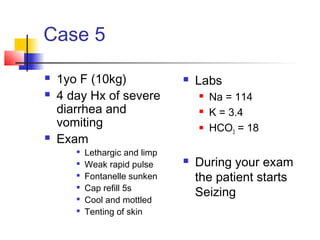
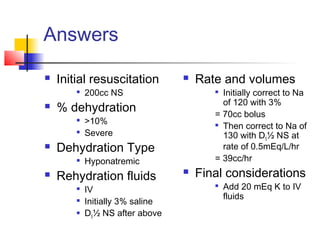


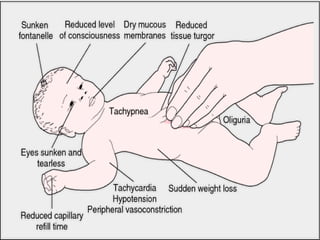
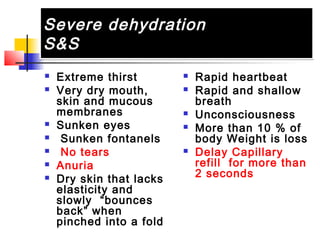
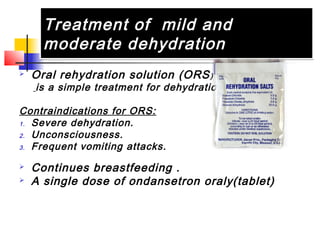
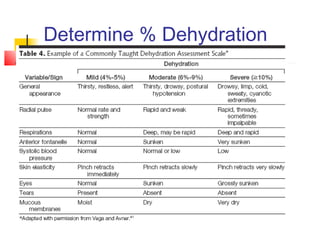
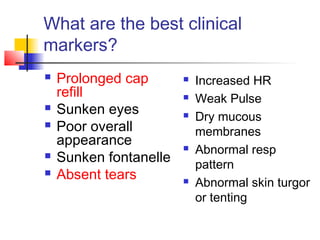
Dehydration is defined as an excessive loss of body fluid and electrolytes where output exceeds input. It can be caused by diarrhea, vomiting, excessive sweating, burns, or blood loss. Dehydration is classified as mild, moderate, or severe based on the total fluid loss as a percentage of body weight. Clinical signs and symptoms vary with the severity of dehydration and can include thirst, dry skin, decreased urine output, drowsiness, and in severe cases, extreme thirst, sunken eyes, and loss of consciousness. Treatment involves oral rehydration for mild to moderate cases and IV fluids for severe dehydration, with the type and rate of fluids dependent on degree of dehydration and electrolyte























































































